
Volume 11, Issue 1 (7-2023)
Jorjani Biomed J 2023, 11(1): 1-2 |
Back to browse issues page

Download citation:
BibTeX | RIS | EndNote | Medlars | ProCite | Reference Manager | RefWorks
Send citation to:



BibTeX | RIS | EndNote | Medlars | ProCite | Reference Manager | RefWorks
Send citation to:
Moudi E, Kamalinia H, Ramezani S, Akbarzade pasha A, Majidi O. A pelvic mass in a 10-year-old boy: a rare diagnosis. Jorjani Biomed J 2023; 11 (1) :1-2
URL: http://goums.ac.ir/jorjanijournal/article-1-914-en.html
URL: http://goums.ac.ir/jorjanijournal/article-1-914-en.html



1- Clinical Research Development Unit of Shahid Beheshti Hospital, Babol University of Medical Sciences, Babol, Iran:Emadmoudi@gmail.com
2- Department of Urology, Babol University of Medical Sciences, Babol, Iran ,hrkamalinia@yahoo.com
3- School of medicine ,faculty of medicine,Babol university of medical science,Mazandaran,Iran
4- Cellular and Molecular Biology Research Center, Health Research Institute, Babol University of Medical Sciences, Babol, Iran
5- Department of Urology, Babol University of Medical Sciences, Babol, Iran
2- Department of Urology, Babol University of Medical Sciences, Babol, Iran ,
3- School of medicine ,faculty of medicine,Babol university of medical science,Mazandaran,Iran
4- Cellular and Molecular Biology Research Center, Health Research Institute, Babol University of Medical Sciences, Babol, Iran
5- Department of Urology, Babol University of Medical Sciences, Babol, Iran
Keywords: Echinococcosis Hepatic, Pelvic
Full-Text [PDF 369 kb]
(1283 Downloads)
| Abstract (HTML) (3275 Views)
Full-Text: (610 Views)
Introduction
Hydatid cyst is a parasitic disease caused by Echinococcus granulosus with a worldwide distribution and is commonly reported in children (1). Dogs are the definitive host of this parasite. Humans can be infected as an intermediate host by consuming unwashed or raw vegetables and ingesting the parasite eggs. The parasite released from the egg reaches the host's body tissues through blood circulation and is localized there (2).
Echinococcus is commonly found within the liver (60%) but can happen anywhere in the body (3). The pelvic organs are seldom the primary location for cyst formation but rather a secondary location for ruptured liver cysts. Pelvic cysts may remain asymptomatic for long periods and may be found accidentally or due to their disturbance and compression symptoms (4). In this report, we narrate a case of pelvic cystic mass that turned out to be a hydatid cyst upon surgical exploration, which is an infrequent primary presentation.
Case Report
A 10-year-old boy was admitted to the clinic with right flank pain. The flank pain has been present for the past two weeks. His family did not recall any previous pain episodes. Past medical history was unremarkable. Physical examination marked a palpable suprapubic mass. His preliminary laboratory tests’ white blood cell count was 7700/μl, with a hemoglobin of 14 g/dl, platelet count of 334000/μl, creatinine level of 0.87 mg/dl, normal urine analysis, and normal liver function tests.
Ultrasonography examination revealed an 81x68 mm cystic lesion behind the pelvis and adjacent to the bladder. Renal ultrasonography reported right renal hydronephrosis.
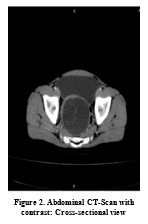
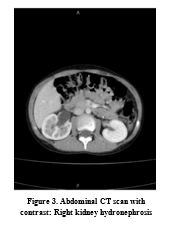
Computed tomography (CT) revealed a cystic lesion located anterior to the sacrum, between the bladder and rectum. The cyst was dimensioned 108´80´60 mm with a relatively thick wall (4mm) that contained internal densities and fine calcification. Furthermore, right renal hydronephrosis and right ureteral dilatation due to the compressive effect of the lesion were reported. (Figures 1, 2).

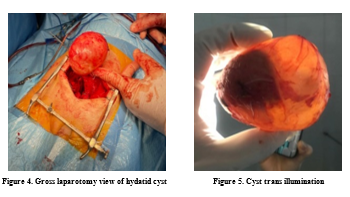
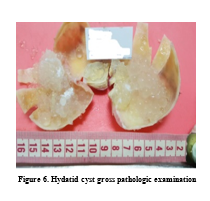
After Paraclinical examinations, the patient underwent surgery with a diagnosis of a seminal vesicle cyst. However, the operation revealed that the lesion was a hydatid cyst (Figures 3, 4). The surgeon removed the hydatid cyst, and the lesion was sent for further pathological examination (Figures 5, 6).
Discussion
A single cyst within the pelvis can be considered primary only when no other cysts are present within the common locales of the event. In such cases, the hydatid embryo gets to the pelvis either through hematogenous or lymphatic dissemination (5). Primary hydatid cysts within the pelvis are very uncommon. The incidence of such lesions is around 0.2 to 0.9 percent. Nearly 80% of all pelvic cases occur in the genital region. Rare cases of primary hydatid cysts have been reported in the pelvis. Most pelvic cysts occur due to the rupture of hydatid cysts in other body parts (6). Primary pelvic echinococcosis appears to be limited to the genital organs that are considered the primary location of inoculation via blood circulation (7, 8). In endemic countries, the crucial factor in diagnosing a hydatid cyst is the awareness of the possibility and clinical suspicion (9). Hydatid cysts should be considered in the differential diagnosis of pelvic masses, especially in children. Ultrasound and CT scans are helpful modalities in investigating any cystic masses or tumors of the pelvis (10).
Acknowledgments
None.
Hydatid cyst is a parasitic disease caused by Echinococcus granulosus with a worldwide distribution and is commonly reported in children (1). Dogs are the definitive host of this parasite. Humans can be infected as an intermediate host by consuming unwashed or raw vegetables and ingesting the parasite eggs. The parasite released from the egg reaches the host's body tissues through blood circulation and is localized there (2).
Echinococcus is commonly found within the liver (60%) but can happen anywhere in the body (3). The pelvic organs are seldom the primary location for cyst formation but rather a secondary location for ruptured liver cysts. Pelvic cysts may remain asymptomatic for long periods and may be found accidentally or due to their disturbance and compression symptoms (4). In this report, we narrate a case of pelvic cystic mass that turned out to be a hydatid cyst upon surgical exploration, which is an infrequent primary presentation.
Case Report
A 10-year-old boy was admitted to the clinic with right flank pain. The flank pain has been present for the past two weeks. His family did not recall any previous pain episodes. Past medical history was unremarkable. Physical examination marked a palpable suprapubic mass. His preliminary laboratory tests’ white blood cell count was 7700/μl, with a hemoglobin of 14 g/dl, platelet count of 334000/μl, creatinine level of 0.87 mg/dl, normal urine analysis, and normal liver function tests.
Ultrasonography examination revealed an 81x68 mm cystic lesion behind the pelvis and adjacent to the bladder. Renal ultrasonography reported right renal hydronephrosis.
Computed tomography (CT) revealed a cystic lesion located anterior to the sacrum, between the bladder and rectum. The cyst was dimensioned 108´80´60 mm with a relatively thick wall (4mm) that contained internal densities and fine calcification. Furthermore, right renal hydronephrosis and right ureteral dilatation due to the compressive effect of the lesion were reported. (Figures 1, 2).
After Paraclinical examinations, the patient underwent surgery with a diagnosis of a seminal vesicle cyst. However, the operation revealed that the lesion was a hydatid cyst (Figures 3, 4). The surgeon removed the hydatid cyst, and the lesion was sent for further pathological examination (Figures 5, 6).
Discussion
A single cyst within the pelvis can be considered primary only when no other cysts are present within the common locales of the event. In such cases, the hydatid embryo gets to the pelvis either through hematogenous or lymphatic dissemination (5). Primary hydatid cysts within the pelvis are very uncommon. The incidence of such lesions is around 0.2 to 0.9 percent. Nearly 80% of all pelvic cases occur in the genital region. Rare cases of primary hydatid cysts have been reported in the pelvis. Most pelvic cysts occur due to the rupture of hydatid cysts in other body parts (6). Primary pelvic echinococcosis appears to be limited to the genital organs that are considered the primary location of inoculation via blood circulation (7, 8). In endemic countries, the crucial factor in diagnosing a hydatid cyst is the awareness of the possibility and clinical suspicion (9). Hydatid cysts should be considered in the differential diagnosis of pelvic masses, especially in children. Ultrasound and CT scans are helpful modalities in investigating any cystic masses or tumors of the pelvis (10).
Acknowledgments
None.
Funding source
Please acknowledge that the surgery and research presented in this manuscript were funded by Babol University of Medical Sciences.Ethical statement
In the methodology section, we want to assure the readers that all ethical considerations were followed. This research received approval from the Babol University of Medical Science Ethical Council, and informed consent was obtained from the patient and their guardian.
Conflict of interest
We affirm that there is no conflict of interest among the authors regarding the publication of this paper.
Author contributions
Dr. Moudi, Dr. Kamalinia, Dr. Akbarzadeh Pasha, and Dr. Majidian played pivotal roles in data collection, patient information gathering, and diagnosing the medical case. Their expertise and insights were crucial to the success of this research, including performing the necessary surgery. Meanwhile, Dr. Ramezani took the lead in writing the essay, interpreting the findings to draw meaningful conclusions.
Type of Article: Case Report |
Subject:
General medicine
Received: 2022/07/2 | Accepted: 2023/02/12 | Published: 2023/07/1
Received: 2022/07/2 | Accepted: 2023/02/12 | Published: 2023/07/1
References
1. Demirci S, Gunaydin G, Dogan KH, Toy H. Sudden death due to hydatid cyst rupture located in right ventricle. The American journal of forensic medicine and pathology. 2008;29(4):346-8. [View at Publisher] [DOI] [PMID] [Google Scholar]
2. Dursun M, Terzibasioglu E, Yilmaz R, Cekrezi B, Olgar S, Nisli K, et al. Cardiac hydatid disease: CT and MRI findings. AJR American journal of roentgenology. 2008;190(1):226-32. [View at Publisher] [DOI] [PMID] [Google Scholar]
3. Bickers WM. Hydatid disease of the female pelvis. American journal of obstetrics and gynecology. 1970;107(3):477-83. [View at Publisher] [DOI] [PMID] [Google Scholar]
4. Aksu MF, Budak E, Ince U, Aksu C. Hydatid cyst of the ovary. Arch Gynecol Obstet. 1997;261(1):51-3. [View at Publisher] [DOI] [PMID] [Google Scholar]
5. Selvaggi FP, Fabiano G, Santacroce S, Traficante A. A retrovesical echinococcal cyst: unusual cause of acute urinary retention. European urology. 1978;4(1):60-2. [View at Publisher] [DOI] [PMID] [Google Scholar]
6. Rahman MS, Rahman J, Lysikiewicz A. Obstetric and gynaecological presentations of hydatid disease. BJOG. 1982;89(8):665-70. [View at Publisher] [DOI] [PMID] [Google Scholar]
7. Cattorini L, Trastulli S, Milani D, Cirocchi R, Giovannelli G, Avenia N, et al. Ovarian hydatid cyst: A case report. Int J Surg Case Rep. 2011;2(6):100-2. [View at Publisher] [DOI] [PMID] [Google Scholar]
8. Zargar-Shoshtari M, Shadpour P, Robat-Moradi N, Moslemi M. Hydatid Cyst of Urinary Tract: 11 Cases at a Single Center. Urology Journal. 2009;4(1):41-5. [View at Publisher] [DOI] [Google scholar]
9. Tehranchi A, Mohammadi bukani H, Modabberi delshad A, Hamedanchi S. Primary Hydatid Cyst of the Kidney in a 10 Year Old Boy. Urology Journal. 2013;10(3):1004-6. [View at Publisher] [PMID] [Google scholar]
10. Díaz-Recaséns J, García-Enguídanos A, Muñoz I, Sáinz de la Cuesta R. Ultrasonographic appearance of an echinococcus ovarian cyst. Obstetrics and gynecology. 1998;91(5 Pt 2):841-2. [View at Publisher] [DOI] [PMID] [Google scholar]
Send email to the article author
| Rights and permissions | |
 |
This work is licensed under a Creative Commons Attribution-NonCommercial 4.0 International License. |
