
Volume 13, Issue 3 (10-2025)
Jorjani Biomed J 2025, 13(3): 37-42 |
Back to browse issues page


Download citation:
BibTeX | RIS | EndNote | Medlars | ProCite | Reference Manager | RefWorks
Send citation to:



BibTeX | RIS | EndNote | Medlars | ProCite | Reference Manager | RefWorks
Send citation to:
Jalilvand M. Motor skill enhancement in children with ADHD: The impact of a targeted sport-based intervention. Jorjani Biomed J 2025; 13 (3) :37-42
URL: http://goums.ac.ir/jorjanijournal/article-1-1097-en.html
URL: http://goums.ac.ir/jorjanijournal/article-1-1097-en.html



Department of Physical Education and Sports Sciences, Ha.C., Islamic Azad University, Hamedan, Iran , jalilvand.mohammad@yahoo.com
Full-Text [PDF 455 kb]
(363 Downloads)
| Abstract (HTML) (2416 Views)
Table 2 presents the results of Levene's test for homogeneity of variances. Levene's test established homogeneity of variances across groups for all dependent measures (Object control: F (1,28) = 0.94, P-Value = 0.338; locomotor skills: F (1,28) = 1.581, P-Value = 0.219; total motor skills: F (1,28) = 3.40, P-Value = 0.075). Box's M test confirmed the homogeneity of covariance matrices assumption for MANCOVA (Box's M = 12.45, P-Value = 0.256). Homogeneity of regression slopes was confirmed. Together, these results indicate that the assumptions of homogeneity of variances and covariance matrices were met for all subsequent analyses.
The baseline characteristics confirmed equivalent demographic profiles between study groups, with no significant differences in age, anthropometric measures, or motor skill scores at pretest (Table 3). Participant characteristics showed no significant between-group differences in age [Experimental: 10.53 ± 0.91 years vs. control: 10.66 ± 1.04 years; t (28) = 0.24, P-Value = 0.812), height (144.20 ± 3.68 cm vs. 144.66 ± 3.43 cm; t (28) = 0.28, P-Value = 0.785), weight (44.46 ± 3.13 kg vs. 45.26 ± 3.08 kg; t (28) = 0.20, P-Value = 0.842), or BMI (21.04 ± 2.44 kg/m2 vs. 21.60 ± 2.74 kg/m2; t(28) = 0.26, P-Value = 0.801].
Discussion
The results of the present study demonstrate that an 8-week table tennis training program produced significant improvements in both locomotor and object control skills in children with ADHD, with particularly large effect sizes for locomotor skills (η2 = 0.80) compared to object control skills (η2 = 0.36). These findings not only confirm the efficacy of targeted sport-based interventions for this population but also extend our understanding of how structured racket sports can address specific motor deficits in ADHD.
When compared with existing literature, our results align with the growing body of evidence supporting physical activity interventions for children with ADHD. The observed improvements in motor skills are consistent with findings from exercise interventions using running programs (30), aerobic exercises (31), and fundamental motor skill training (19). Supporting this pattern, Eskandarnejad, Jahedi Khajeh, and Rezaee (32) demonstrated that basketball training improved motor skills in boys with ADHD, while Keykhahosseinpour et al. (33) reported significant improvements in motor coordination following aerobic exercise and group play therapy. However, our study extends this literature by specifically investigating table tennis as a targeted intervention, whereas previous research has primarily focused on general physical activities or clinical rehabilitation exercises.
The particularly strong effects on locomotor skills (η2 = 0.80) compared to object control skills (η2 = 0.36) warrant special attention. This differential improvement pattern aligns with table tennis's unique demands for dynamic balance, rapid weight shifting, and whole-body coordination - precisely the domains most impaired in children with ADHD (6,34). While direct comparisons are limited, the magnitude of improvement in locomotor skills aligns with the notion that targeted sports interventions can produce substantial effects when they directly address core deficits in specific populations. The specificity of table tennis to locomotor requirements, combined with the game-based format that enhanced participant engagement, may explain why our intervention yielded particularly strong effects in this domain. Additionally, the remarkably large effect sizes should be interpreted cautiously within our specific methodological context and require independent replication in larger, more diverse samples.
Regarding the potential mechanisms underlying these improvements, several interrelated factors likely contributed to our positive outcomes. Table tennis inherently requires sophisticated perceptual-motor integration and visual tracking (35,36), functions that are often compromised in children with ADHD. The sport's demand for anticipating ball trajectory, adjusting body position in response to changing stimuli, and executing precise strokes necessarily strengthens fundamental motor competencies (37,38). This perspective is supported by Bashiri, Farsi, Abdoli, and Kavyani (25), who found table tennis training significantly enhanced reaction time, anticipatory timing, and hand-eye coordination, while Virgens Chagas, Macedo, and Batista (23) emphasized the sport's potential for improving overall motor coordination levels.
From a neurobiological perspective, table tennis induces multifaceted beneficial changes in brain function that support motor learning and execution. As an open-skill aerobic activity requiring sustained attention and rapid motor responses, it promotes neurotransmitter systems crucial for motor control. Notably, open-skill sports like basketball and table tennis enhance perceptual-motor coordination through combined cardiorespiratory fitness and rich environmental stimuli, increasing Purkinje neuron connectivity, promoting prefrontal cortex vascularization, and inducing neural reorganization (39). Additionally, table tennis activates sensorimotor and visual-spatial networks while increasing serotonin and dopamine secretion, improving cerebral circulation, enhancing brain metabolism, and strengthening BDNF synthesis to support neural plasticity (15). This comprehensive neurobiological impact aligns with the dynamic nature of table tennis, which Visser, Büchel, Lehmann, and Baumeister (40) identified as particularly beneficial for brain function due to its continuous demands for environmental adaptation.
The cognitive benefits of table tennis extend beyond motor domains, as demonstrated by Chen, Tsai, Wang, and Wuang (37), who found improved visual perception and executive functions in children with intellectual disabilities following table tennis training. Similarly, Pan et al. (38) documented enhanced focus and attention, while Pan et al. (24) highlighted the sport's engagement of prefrontal and cerebellar networks implicated in ADHD pathophysiology. These cognitive-motor interactions likely contributed to our observed motor improvements, as efficient motor performance depends on adequate cognitive control.
Beyond the immediate benefits, our findings have important practical implications. The game-based format of table tennis proved highly engaging for children with ADHD, as reflected in our 95% adherence rate. This is particularly significant given that children with ADHD typically engage in less physical activity than their peers (18), and our approach successfully addressed this participation gap. The accessibility and enjoyment of table tennis, coupled with its minimal equipment requirements, make it a feasible and sustainable intervention for various settings, from clinical rehabilitation to school physical education programs.
Despite these promising findings, several limitations must be acknowledged. The exclusive focus on male participants limits the generalizability of our findings to females with ADHD. Furthermore, the absence of follow-up assessments prevents conclusions about the long-term maintenance of acquired motor skills. Most notably, we did not measure potential changes in cognitive functions or ADHD core symptoms despite table tennis's documented benefits for executive functions, preventing examination of whether motor improvements translated into broader functional gains. Additionally, the remarkably large effect sizes should be interpreted cautiously within our specific methodological context.
Future research should therefore investigate table tennis training in larger, more diverse samples including female participants, incorporate comprehensive assessment batteries measuring cognitive functions and ADHD symptom severity, and implement longitudinal designs with follow-up assessments. Building on previous methodology, researchers could adapt protocols from Tsai, Wang, and Tseng (27) and Jalilvand and Azadian (29) while addressing the identified limitations. Studies should also explore transfer effects to academic performance and social functioning, and investigate optimal training parameters for different ADHD presentations.
Conclusion
This study provides compelling evidence that structured table tennis training effectively improves fundamental motor skills in children with ADHD, with particularly strong effects on locomotor abilities. The differential impact across motor domains, high adherence rates, and multi-system benefits support integrating targeted racket sports into comprehensive treatment approaches. Based on our findings and consistent with previous research, we recommend that clinicians, educators, and parents consider incorporating table tennis into regular activity routines while researchers continue to explore the optimal parameters and broader benefits of such interventions.
Acknowledgement
The author sincerely appreciates the valuable assistance and support of all individuals who contributed to this research.
Funding sources
This research received no specific grant from any funding agency in the public, commercial, or not-for-profit sectors.
Ethical statement
This study was conducted in accordance with the ethical principles outlined in the Declaration of Helsinki. Ethical approval was granted by the Islamic Azad University Human Research Ethics Committee (Approval code: IR.IAU.H.REC.1403.039).
Conflicts of interest
The author declares no conflict of interest.
Author contributions
The author was solely responsible for all aspects of the study, including conception, design, data collection, analysis, and manuscript preparation.
Data availability statement
The data that support the findings of this study are available from the corresponding author upon reasonable request.
Full-Text: (70 Views)
Introduction
Attention Deficit Hyperactivity Disorder (ADHD) is a neurodevelopmental disorder characterized by persistent patterns of inattention, hyperactivity, and impulsivity, leading to varying degrees of functional impairment (1). Recognized as one of the most prevalent neurodevelopmental disorders, ADHD affects 5-7% of children worldwide, depending on diagnostic criteria (2), with recent evidence indicating a rising global prevalence among children and adolescents (3). ADHD pathogenesis involves a complex interaction between genetic susceptibility and environmental factors, with each component making modest but cumulative contributions. The heritability of ADHD has been well-established. Additional risk factors include perinatal injuries, infectious diseases, nutritional status, atopic conditions (Such as allergies, eczema, and asthma), sleep disturbances, and childhood corticosteroid use - all associated with the onset and severity of hyperactive symptoms (4).
Current neurobiological explanations focus on frontal lobe impairments. The prefrontal hypothesis posits that cortical regions governing cognitive functions are dysfunctional in individuals with ADHD (5). Beyond these cognitive manifestations, motor hyperactivity constitutes a core feature of ADHD, manifesting as excessive movements and physical restlessness. Children with ADHD demonstrate both fine and gross motor deficits, exhibiting particular difficulties with ball skills, balance, and locomotor abilities compared to neurotypical peers (6). These motor impairments often underlie secondary academic and social functioning difficulties (6,7), specifically contributing to challenges with handwriting, participation in physical education, and the execution of classroom tasks requiring fine motor control and coordination (6).
Given these multifaceted challenges, international clinical practice guidelines recommend combined pharmacological and non-pharmacological interventions for ADHD management (7-9). While medications provide short-term benefits for core symptoms and improve daily functioning-particularly in academic settings-their long-term effects remain unclear. Furthermore, stimulant medications carry well-documented adverse effects including appetite suppression, abdominal pain, mood disturbances, sleep problems, headaches, and potential growth delays at higher dosages (10,11). These pharmaceutical side effects have prompted growing concern among parents and caregivers, driving interest in non-drug alternatives.
In direct response to these concerns and preferences, various non-pharmacological interventions have been developed as complementary or alternative approaches. These include behavioral parent training, cognitive training, neurofeedback, and dietary modifications (12). Among these alternatives, physical exercise has gained prominence as a particularly accessible and low-risk intervention. Compared to other non-pharmacological options, structured physical activity offers a unique advantage by simultaneously targeting multiple core deficits in ADHD. It not only addresses motor proficiency but also directly enhances cognitive functions such as attention and executive control, which are often impaired in children with ADHD (13,14). Furthermore, exercise induces beneficial neurobiological changes, including increased dopamine and norepinephrine activity-similar to stimulant medications but without the adverse side effects-and promotes brain-derived neurotrophic factor (BDNF) synthesis, which supports neural plasticity and cognitive improvement (15).
Collectively, this multi-systemic impact makes physical exercise a particularly comprehensive and efficient non-pharmacological intervention for managing both motor and cognitive symptoms in children with ADHD (13,14).
Studies indicate that the impact of exercise and physical activity on motor outcomes is influenced by various factors, including the type and intensity of activity, duration of implementation, and the specific population under investigation (15). Most physical activities or exercise interventions for children with attention deficit hyperactivity disorder consist of clinical rehabilitation exercises aimed at improving motor coordination, cognitive functioning, and interpersonal skills or emotional disorders (14). Both acute exercise and regular physical activity can induce physiological and psychological mechanisms that not only enhance physical and mental health but also improve physiological and cognitive functions in these children (16). Furthermore, based on the symptoms of attention deficit hyperactivity disorder (Impulsivity and hyperactivity), combining exercise training with conventional treatments enhances the benefits of intervention (17).
Despite this compelling evidence about physical activity, children with ADHD engage in less physical activity than their non-ADHD peers (18), highlighting the critical need for engaging, sport-based interventions that can motivate sustained participation. Some research demonstrates the positive impact of physical activity on various developmental domains in hyperactive children. For example, Najafi Shahna, Dinan, and Ahmadpour (19) demonstrated that fundamental motor skill training significantly improved both motor and cognitive skills in children with attention deficit hyperactivity disorder. Similarly, the results of Rasoolyar and Jalilvand (20) demonstrated the positive effects of yoga exercises on static and dynamic balance in children with ADHD. Furthermore, Feng, Li, Yong, and Tian (21) found that after participating in sports activities, the motor skill levels of hyperactive children improved significantly.
Unlike the general sports activities previously mentioned, table tennis has been introduced as a globally prominent sport for children (22). Racket sports, including table tennis, rank among the most popular choices for boys, following team sports and martial arts. Performing this sport requires substantial sensorimotor and cognitive demands while simultaneously depending on both manipulative and locomotor skills for successful execution. Table tennis represents an open and complex motor skill performed with high ball velocity in a dynamic and unpredictable environment. Skilled performance in table tennis correlates with various types of motor skills. Given these characteristics and evidence, table tennis is expected to significantly improve motor coordination levels (23). Table tennis is a comprehensive sport that enhances both upper and lower body musculature, strengthens the cardiorespiratory system, and positively impacts motor skills and executive functions (22). This sport can serve as an effective strategy to motivate children and adolescents toward regular physical activity participation, achieving desirable health outcomes and reducing sedentary behavior. Furthermore, table tennis necessitates visual tracking capability and the use of predictive control mechanisms governed by the prefrontal cortex and cerebellum - cortical regions associated with cognitive functions in individuals with ADHD (24).
However, despite these promising characteristics, studies such as that of Bashiri et al. (25) have demonstrated the benefits of table tennis for perceptual-motor skills in typically developing children. These findings cannot be directly generalized to children with ADHD due to their distinct motor profiles and needs (26). This is particularly concerning given the current lack of specific, movement-based intervention guidelines for addressing motor deficits in this population (7). Therefore, to bridge this critical gap, the present study aimed to evaluate the effectiveness of a targeted 8-week table tennis training program on fundamental motor skills in children with ADHD. The findings are expected to provide crucial scientific evidence for developing structured, sport-based motor interventions tailored to this clinical population, ultimately contributing to improved quality of life.
Methods
Participants
The present study employed a quasi-experimental design with pretest-posttest and control group. The research was conducted on a statistical population of male students aged 9 - 12 years with attention deficit hyperactivity disorder (ADHD) in Hamedan during the 2023 - 2024 academic year, whose diagnosis had been confirmed by a specialist psychiatrist based on DSM-5 criteria. From 85 volunteer families recruited through announcements in schools and treatment centers, 45 children met the inclusion criteria after initial screening: (1) Confirmed ADHD diagnosis, (2) age range 9-12 years, (3) no stimulant medication use, (4) absence of comorbid disorders such as autism or intellectual disability, and (5) scoring above 34 on the Conners' Parent Rating Scale. Of these, 32 families provided informed consent. Considering a potential 15% attrition rate and based on sample size calculation in G Power software (Assuming medium effect size of 0.5, significance level of 0.05, and statistical power of 0.8), 30 participants were ultimately randomly assigned (Based on age and symptom severity) into two 15-member experimental and control groups. To maintain ethical principles, all families were assured of their right to withdraw at any stage.
Procedure
Prior to the study, ethical approval was obtained (Code: IR.IAU.H.REC.1403.039). After providing informed consent, all participants completed demographic forms and attended an orientation session. Baseline assessments included measurements of height, weight, and BMI, followed by a pretest of motor skills using the Test of Gross Motor Development-3 (TGMD-3). The participants were then allocated to either the experimental or control group using block randomization, which was stratified based on age, disorder severity, and pretest motor scores.
The experimental group underwent an 8-week table tennis training program, consisting of three 60-minute sessions per week in a sports hall. Sessions were supervised by a certified coach specializing in child instruction, assisted by two aides. Each session followed a structured protocol comprising four components: A warm-up, instruction in basic table tennis skills, gameplay, and a cool-down period. A detailed operational guide standardized the duration and content of each component, as well as coaching instructions.
Training progression began with fundamental skills (Proper racket grip, stance, and forehand/backhand movements) and advanced to serving techniques, targeted drills, and both singles and doubles match play. Perceptual-motor exercises were integrated to enhance eye-hand coordination, decision-making speed, focus, reaction time, visual perception, and inhibitory control. These activities, which required attentive responses to coach instructions and color-coded ball stimuli, included: Differential catching and hitting of white versus orange balls; responding selectively to even-numbered balls; and returning serves of varying speed, direction, and difficulty. All exercises were delivered in game-like formats, with complexity individually tailored to each child's motor abilities. The intervention protocol was adapted from established studies (24,27-29). To ensure treatment fidelity, an independent observer used a daily checklist to monitor adherence (95% overall), assessing session duration, quality of instruction, and participant engagement.
Following the 8-week intervention, all participants completed the TGMD-3 as a post-test within 48 - 72 hours. To maintain blinding, two trained assessors who were unaware of group assignments and absent during the intervention sessions conducted all scoring. Inter-rater reliability was excellent, with a correlation coefficient exceeding 0.9 between the independent assessors' scores. Furthermore, throughout the study period, researchers maintained weekly contact with physical education teachers and parents to monitor and ensure that no children participated in extracurricular sports or concurrent motor rehabilitation programs.
Research instruments
Conners' ADHD rating scale
To assess the level of attention deficit and hyperactivity in children, the parent version of the Conners' Attention Deficit Hyperactivity Disorder (ADHD) Rating Scale was used. The Conners' ADHD Rating Scale is a 26-item questionnaire scored on a Likert scale. For each item, parents select one of the options from 1 to 4 ("never," "sometimes," "often," or "very often") based on their child's symptoms. The total score ranges from 26 to 104, and according to the questionnaire's interpretation guidelines, a score of 34 or higher indicates the presence of the disorder. The validity and reliability of this scale have been reported as satisfactory.
Ulrich motor development test (TGMD-3)
In the present study, the third edition of the Ulrich Motor Development Test (TGMD-3) was used to assess children's motor skills. This test consists of two subscales: The locomotor skills subscale and the object control (Manipulative skills) subscale. Out of a total possible score of 100 on the TGMD-3, the locomotor skills subscale accounts for 46 points, while the object control subscale accounts for 54 points. The validity and reliability of this test have been reported as satisfactory.
Data analyses
For data analysis, descriptive statistics (Measures of central tendency and dispersion) were used initially. The Shapiro-Wilk test was employed to examine data normality. Finally, paired t-tests and analysis of covariance (ANCOVA) were conducted using SPSS version 19 to test the research hypotheses, with the significance level set at 0.05 for all analyses.
Results
Prior to conducting primary analyses, all statistical assumptions were thoroughly examined. The Shapiro-Wilk test confirmed normality of distribution for all variables at both pre-test and post-test assessments (All P > 0.05, Table 1).
Attention Deficit Hyperactivity Disorder (ADHD) is a neurodevelopmental disorder characterized by persistent patterns of inattention, hyperactivity, and impulsivity, leading to varying degrees of functional impairment (1). Recognized as one of the most prevalent neurodevelopmental disorders, ADHD affects 5-7% of children worldwide, depending on diagnostic criteria (2), with recent evidence indicating a rising global prevalence among children and adolescents (3). ADHD pathogenesis involves a complex interaction between genetic susceptibility and environmental factors, with each component making modest but cumulative contributions. The heritability of ADHD has been well-established. Additional risk factors include perinatal injuries, infectious diseases, nutritional status, atopic conditions (Such as allergies, eczema, and asthma), sleep disturbances, and childhood corticosteroid use - all associated with the onset and severity of hyperactive symptoms (4).
Current neurobiological explanations focus on frontal lobe impairments. The prefrontal hypothesis posits that cortical regions governing cognitive functions are dysfunctional in individuals with ADHD (5). Beyond these cognitive manifestations, motor hyperactivity constitutes a core feature of ADHD, manifesting as excessive movements and physical restlessness. Children with ADHD demonstrate both fine and gross motor deficits, exhibiting particular difficulties with ball skills, balance, and locomotor abilities compared to neurotypical peers (6). These motor impairments often underlie secondary academic and social functioning difficulties (6,7), specifically contributing to challenges with handwriting, participation in physical education, and the execution of classroom tasks requiring fine motor control and coordination (6).
Given these multifaceted challenges, international clinical practice guidelines recommend combined pharmacological and non-pharmacological interventions for ADHD management (7-9). While medications provide short-term benefits for core symptoms and improve daily functioning-particularly in academic settings-their long-term effects remain unclear. Furthermore, stimulant medications carry well-documented adverse effects including appetite suppression, abdominal pain, mood disturbances, sleep problems, headaches, and potential growth delays at higher dosages (10,11). These pharmaceutical side effects have prompted growing concern among parents and caregivers, driving interest in non-drug alternatives.
In direct response to these concerns and preferences, various non-pharmacological interventions have been developed as complementary or alternative approaches. These include behavioral parent training, cognitive training, neurofeedback, and dietary modifications (12). Among these alternatives, physical exercise has gained prominence as a particularly accessible and low-risk intervention. Compared to other non-pharmacological options, structured physical activity offers a unique advantage by simultaneously targeting multiple core deficits in ADHD. It not only addresses motor proficiency but also directly enhances cognitive functions such as attention and executive control, which are often impaired in children with ADHD (13,14). Furthermore, exercise induces beneficial neurobiological changes, including increased dopamine and norepinephrine activity-similar to stimulant medications but without the adverse side effects-and promotes brain-derived neurotrophic factor (BDNF) synthesis, which supports neural plasticity and cognitive improvement (15).
Collectively, this multi-systemic impact makes physical exercise a particularly comprehensive and efficient non-pharmacological intervention for managing both motor and cognitive symptoms in children with ADHD (13,14).
Studies indicate that the impact of exercise and physical activity on motor outcomes is influenced by various factors, including the type and intensity of activity, duration of implementation, and the specific population under investigation (15). Most physical activities or exercise interventions for children with attention deficit hyperactivity disorder consist of clinical rehabilitation exercises aimed at improving motor coordination, cognitive functioning, and interpersonal skills or emotional disorders (14). Both acute exercise and regular physical activity can induce physiological and psychological mechanisms that not only enhance physical and mental health but also improve physiological and cognitive functions in these children (16). Furthermore, based on the symptoms of attention deficit hyperactivity disorder (Impulsivity and hyperactivity), combining exercise training with conventional treatments enhances the benefits of intervention (17).
Despite this compelling evidence about physical activity, children with ADHD engage in less physical activity than their non-ADHD peers (18), highlighting the critical need for engaging, sport-based interventions that can motivate sustained participation. Some research demonstrates the positive impact of physical activity on various developmental domains in hyperactive children. For example, Najafi Shahna, Dinan, and Ahmadpour (19) demonstrated that fundamental motor skill training significantly improved both motor and cognitive skills in children with attention deficit hyperactivity disorder. Similarly, the results of Rasoolyar and Jalilvand (20) demonstrated the positive effects of yoga exercises on static and dynamic balance in children with ADHD. Furthermore, Feng, Li, Yong, and Tian (21) found that after participating in sports activities, the motor skill levels of hyperactive children improved significantly.
Unlike the general sports activities previously mentioned, table tennis has been introduced as a globally prominent sport for children (22). Racket sports, including table tennis, rank among the most popular choices for boys, following team sports and martial arts. Performing this sport requires substantial sensorimotor and cognitive demands while simultaneously depending on both manipulative and locomotor skills for successful execution. Table tennis represents an open and complex motor skill performed with high ball velocity in a dynamic and unpredictable environment. Skilled performance in table tennis correlates with various types of motor skills. Given these characteristics and evidence, table tennis is expected to significantly improve motor coordination levels (23). Table tennis is a comprehensive sport that enhances both upper and lower body musculature, strengthens the cardiorespiratory system, and positively impacts motor skills and executive functions (22). This sport can serve as an effective strategy to motivate children and adolescents toward regular physical activity participation, achieving desirable health outcomes and reducing sedentary behavior. Furthermore, table tennis necessitates visual tracking capability and the use of predictive control mechanisms governed by the prefrontal cortex and cerebellum - cortical regions associated with cognitive functions in individuals with ADHD (24).
However, despite these promising characteristics, studies such as that of Bashiri et al. (25) have demonstrated the benefits of table tennis for perceptual-motor skills in typically developing children. These findings cannot be directly generalized to children with ADHD due to their distinct motor profiles and needs (26). This is particularly concerning given the current lack of specific, movement-based intervention guidelines for addressing motor deficits in this population (7). Therefore, to bridge this critical gap, the present study aimed to evaluate the effectiveness of a targeted 8-week table tennis training program on fundamental motor skills in children with ADHD. The findings are expected to provide crucial scientific evidence for developing structured, sport-based motor interventions tailored to this clinical population, ultimately contributing to improved quality of life.
Methods
Participants
The present study employed a quasi-experimental design with pretest-posttest and control group. The research was conducted on a statistical population of male students aged 9 - 12 years with attention deficit hyperactivity disorder (ADHD) in Hamedan during the 2023 - 2024 academic year, whose diagnosis had been confirmed by a specialist psychiatrist based on DSM-5 criteria. From 85 volunteer families recruited through announcements in schools and treatment centers, 45 children met the inclusion criteria after initial screening: (1) Confirmed ADHD diagnosis, (2) age range 9-12 years, (3) no stimulant medication use, (4) absence of comorbid disorders such as autism or intellectual disability, and (5) scoring above 34 on the Conners' Parent Rating Scale. Of these, 32 families provided informed consent. Considering a potential 15% attrition rate and based on sample size calculation in G Power software (Assuming medium effect size of 0.5, significance level of 0.05, and statistical power of 0.8), 30 participants were ultimately randomly assigned (Based on age and symptom severity) into two 15-member experimental and control groups. To maintain ethical principles, all families were assured of their right to withdraw at any stage.
Procedure
Prior to the study, ethical approval was obtained (Code: IR.IAU.H.REC.1403.039). After providing informed consent, all participants completed demographic forms and attended an orientation session. Baseline assessments included measurements of height, weight, and BMI, followed by a pretest of motor skills using the Test of Gross Motor Development-3 (TGMD-3). The participants were then allocated to either the experimental or control group using block randomization, which was stratified based on age, disorder severity, and pretest motor scores.
The experimental group underwent an 8-week table tennis training program, consisting of three 60-minute sessions per week in a sports hall. Sessions were supervised by a certified coach specializing in child instruction, assisted by two aides. Each session followed a structured protocol comprising four components: A warm-up, instruction in basic table tennis skills, gameplay, and a cool-down period. A detailed operational guide standardized the duration and content of each component, as well as coaching instructions.
Training progression began with fundamental skills (Proper racket grip, stance, and forehand/backhand movements) and advanced to serving techniques, targeted drills, and both singles and doubles match play. Perceptual-motor exercises were integrated to enhance eye-hand coordination, decision-making speed, focus, reaction time, visual perception, and inhibitory control. These activities, which required attentive responses to coach instructions and color-coded ball stimuli, included: Differential catching and hitting of white versus orange balls; responding selectively to even-numbered balls; and returning serves of varying speed, direction, and difficulty. All exercises were delivered in game-like formats, with complexity individually tailored to each child's motor abilities. The intervention protocol was adapted from established studies (24,27-29). To ensure treatment fidelity, an independent observer used a daily checklist to monitor adherence (95% overall), assessing session duration, quality of instruction, and participant engagement.
Following the 8-week intervention, all participants completed the TGMD-3 as a post-test within 48 - 72 hours. To maintain blinding, two trained assessors who were unaware of group assignments and absent during the intervention sessions conducted all scoring. Inter-rater reliability was excellent, with a correlation coefficient exceeding 0.9 between the independent assessors' scores. Furthermore, throughout the study period, researchers maintained weekly contact with physical education teachers and parents to monitor and ensure that no children participated in extracurricular sports or concurrent motor rehabilitation programs.
Research instruments
Conners' ADHD rating scale
To assess the level of attention deficit and hyperactivity in children, the parent version of the Conners' Attention Deficit Hyperactivity Disorder (ADHD) Rating Scale was used. The Conners' ADHD Rating Scale is a 26-item questionnaire scored on a Likert scale. For each item, parents select one of the options from 1 to 4 ("never," "sometimes," "often," or "very often") based on their child's symptoms. The total score ranges from 26 to 104, and according to the questionnaire's interpretation guidelines, a score of 34 or higher indicates the presence of the disorder. The validity and reliability of this scale have been reported as satisfactory.
Ulrich motor development test (TGMD-3)
In the present study, the third edition of the Ulrich Motor Development Test (TGMD-3) was used to assess children's motor skills. This test consists of two subscales: The locomotor skills subscale and the object control (Manipulative skills) subscale. Out of a total possible score of 100 on the TGMD-3, the locomotor skills subscale accounts for 46 points, while the object control subscale accounts for 54 points. The validity and reliability of this test have been reported as satisfactory.
Data analyses
For data analysis, descriptive statistics (Measures of central tendency and dispersion) were used initially. The Shapiro-Wilk test was employed to examine data normality. Finally, paired t-tests and analysis of covariance (ANCOVA) were conducted using SPSS version 19 to test the research hypotheses, with the significance level set at 0.05 for all analyses.
Results
Prior to conducting primary analyses, all statistical assumptions were thoroughly examined. The Shapiro-Wilk test confirmed normality of distribution for all variables at both pre-test and post-test assessments (All P > 0.05, Table 1).
|
Table 1. Normality tests using Shapiro-wilk test
 |
The baseline characteristics confirmed equivalent demographic profiles between study groups, with no significant differences in age, anthropometric measures, or motor skill scores at pretest (Table 3). Participant characteristics showed no significant between-group differences in age [Experimental: 10.53 ± 0.91 years vs. control: 10.66 ± 1.04 years; t (28) = 0.24, P-Value = 0.812), height (144.20 ± 3.68 cm vs. 144.66 ± 3.43 cm; t (28) = 0.28, P-Value = 0.785), weight (44.46 ± 3.13 kg vs. 45.26 ± 3.08 kg; t (28) = 0.20, P-Value = 0.842), or BMI (21.04 ± 2.44 kg/m2 vs. 21.60 ± 2.74 kg/m2; t(28) = 0.26, P-Value = 0.801].
Paired t-tests revealed significant improvements in the experimental group across all motor skill assessments compared to controls (Table 4). The experimental group showed significant improvement in object control skills (25.40 ± 1.91 to 29.93 ± 2.49; t (14) = 10.14, P-Value < 0.001, d = 2.12) and locomotor skills (27.93 ± 1.90 to 31.33 ± 2.29; t (14) = 16.56, P-Value < 0.001, d = 1.89), while control group changes were nonsignificant (Object control: 25.26 ± 1.66 to 25.97 ± 1.59, P-Value = 0.061; locomotor: 28.33 ± 1.71 to 28.73 ± 2.08, P-Value = 0.479). Total motor scores increased substantially in the experimental group (53.33 ± 3.47 to 61.26 ± 4.13; t (14) = 29.75, P-Value < 0.001, d = 2.34) versus minimal control group change (53.66 ± 2.91 to 54.10 ± 2.73, P-Value = 0.425).
|
Table 3. Baseline demographic and anthropometric characteristics
 Note: Independent t-tests showed no significant differences between groups at baseline (All P-value > 0.05). |
Figure 1, including the pre- and post-test scores for object control, locomotor skills, and total motor performance in the experimental and control groups.
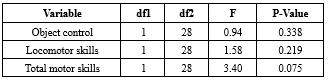
To test research hypotheses, one-way multivariate analysis of covariance (MANCOVA) was conducted as the primary analysis to evaluate the overall intervention effect on the combined motor skill variables (Object control, locomotor skills, and total motor score), using the respective pre‑test scores as covariates. This approach was selected because the three primary outcome measures-object control skills, locomotor skills, and total motor score-are theoretically and empirically correlated. Conducting separate univariate analyses would increase the risk of Type I error. Therefore, MANCOVA was employed to evaluate the overall intervention effect on this set of related dependent variables while adjusting for baseline (pre‑test) scores, providing a more powerful and statistically appropriate analysis (Table 5). Assumption testing confirmed homogeneity of covariance matrices and regression slopes (All P-Value > 0.05). The analysis revealed a significant multivariate effect (Pillai's Trace = 0.91, F (3, 25) = 78.57, P-Value < 0.001, partial η2 = 0.91), indicating that the intervention accounted for 91.1% of the variance in post-test motor performance. The estimated marginal means for each group, adjusted for pre-test covariates, were as follows: for the experimental group, object control = 29.90, locomotor skills = 31.59, and total motor score = 61.49; for the control group, object control = 24.57, locomotor skills = 28.48, total motor score = 52.98.
To test research hypotheses, one-way multivariate analysis of covariance (MANCOVA) was conducted as the primary analysis to evaluate the overall intervention effect on the combined motor skill variables (Object control, locomotor skills, and total motor score), using the respective pre‑test scores as covariates. This approach was selected because the three primary outcome measures-object control skills, locomotor skills, and total motor score-are theoretically and empirically correlated. Conducting separate univariate analyses would increase the risk of Type I error. Therefore, MANCOVA was employed to evaluate the overall intervention effect on this set of related dependent variables while adjusting for baseline (pre‑test) scores, providing a more powerful and statistically appropriate analysis (Table 5). Assumption testing confirmed homogeneity of covariance matrices and regression slopes (All P-Value > 0.05). The analysis revealed a significant multivariate effect (Pillai's Trace = 0.91, F (3, 25) = 78.57, P-Value < 0.001, partial η2 = 0.91), indicating that the intervention accounted for 91.1% of the variance in post-test motor performance. The estimated marginal means for each group, adjusted for pre-test covariates, were as follows: for the experimental group, object control = 29.90, locomotor skills = 31.59, and total motor score = 61.49; for the control group, object control = 24.57, locomotor skills = 28.48, total motor score = 52.98.
|
Table 4. Pre-post intervention comparisons of motor skills
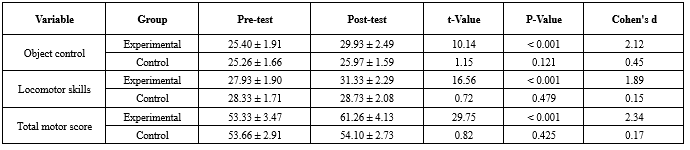 |
 Figure 1. Pre- and post-test scores for object control, locomotor skills, and total motor performance in experimental and control groups |
Following this significant omnibus result, protected univariate ANCOVAs were conducted (Table 6), revealing significant effects for locomotor skills [F(1, 27) = 108.54, P-Value < 0.001, partial η2 = 0.801], object control [F(1, 27) = 15.21, P-Value < 0.001, partial η2 = 0.360], and total motor score [F(1, 27) = 86.06, P-Value < 0.001, partial η2 = 0.761].


Discussion
The results of the present study demonstrate that an 8-week table tennis training program produced significant improvements in both locomotor and object control skills in children with ADHD, with particularly large effect sizes for locomotor skills (η2 = 0.80) compared to object control skills (η2 = 0.36). These findings not only confirm the efficacy of targeted sport-based interventions for this population but also extend our understanding of how structured racket sports can address specific motor deficits in ADHD.
When compared with existing literature, our results align with the growing body of evidence supporting physical activity interventions for children with ADHD. The observed improvements in motor skills are consistent with findings from exercise interventions using running programs (30), aerobic exercises (31), and fundamental motor skill training (19). Supporting this pattern, Eskandarnejad, Jahedi Khajeh, and Rezaee (32) demonstrated that basketball training improved motor skills in boys with ADHD, while Keykhahosseinpour et al. (33) reported significant improvements in motor coordination following aerobic exercise and group play therapy. However, our study extends this literature by specifically investigating table tennis as a targeted intervention, whereas previous research has primarily focused on general physical activities or clinical rehabilitation exercises.
The particularly strong effects on locomotor skills (η2 = 0.80) compared to object control skills (η2 = 0.36) warrant special attention. This differential improvement pattern aligns with table tennis's unique demands for dynamic balance, rapid weight shifting, and whole-body coordination - precisely the domains most impaired in children with ADHD (6,34). While direct comparisons are limited, the magnitude of improvement in locomotor skills aligns with the notion that targeted sports interventions can produce substantial effects when they directly address core deficits in specific populations. The specificity of table tennis to locomotor requirements, combined with the game-based format that enhanced participant engagement, may explain why our intervention yielded particularly strong effects in this domain. Additionally, the remarkably large effect sizes should be interpreted cautiously within our specific methodological context and require independent replication in larger, more diverse samples.
Regarding the potential mechanisms underlying these improvements, several interrelated factors likely contributed to our positive outcomes. Table tennis inherently requires sophisticated perceptual-motor integration and visual tracking (35,36), functions that are often compromised in children with ADHD. The sport's demand for anticipating ball trajectory, adjusting body position in response to changing stimuli, and executing precise strokes necessarily strengthens fundamental motor competencies (37,38). This perspective is supported by Bashiri, Farsi, Abdoli, and Kavyani (25), who found table tennis training significantly enhanced reaction time, anticipatory timing, and hand-eye coordination, while Virgens Chagas, Macedo, and Batista (23) emphasized the sport's potential for improving overall motor coordination levels.
From a neurobiological perspective, table tennis induces multifaceted beneficial changes in brain function that support motor learning and execution. As an open-skill aerobic activity requiring sustained attention and rapid motor responses, it promotes neurotransmitter systems crucial for motor control. Notably, open-skill sports like basketball and table tennis enhance perceptual-motor coordination through combined cardiorespiratory fitness and rich environmental stimuli, increasing Purkinje neuron connectivity, promoting prefrontal cortex vascularization, and inducing neural reorganization (39). Additionally, table tennis activates sensorimotor and visual-spatial networks while increasing serotonin and dopamine secretion, improving cerebral circulation, enhancing brain metabolism, and strengthening BDNF synthesis to support neural plasticity (15). This comprehensive neurobiological impact aligns with the dynamic nature of table tennis, which Visser, Büchel, Lehmann, and Baumeister (40) identified as particularly beneficial for brain function due to its continuous demands for environmental adaptation.
The cognitive benefits of table tennis extend beyond motor domains, as demonstrated by Chen, Tsai, Wang, and Wuang (37), who found improved visual perception and executive functions in children with intellectual disabilities following table tennis training. Similarly, Pan et al. (38) documented enhanced focus and attention, while Pan et al. (24) highlighted the sport's engagement of prefrontal and cerebellar networks implicated in ADHD pathophysiology. These cognitive-motor interactions likely contributed to our observed motor improvements, as efficient motor performance depends on adequate cognitive control.
Beyond the immediate benefits, our findings have important practical implications. The game-based format of table tennis proved highly engaging for children with ADHD, as reflected in our 95% adherence rate. This is particularly significant given that children with ADHD typically engage in less physical activity than their peers (18), and our approach successfully addressed this participation gap. The accessibility and enjoyment of table tennis, coupled with its minimal equipment requirements, make it a feasible and sustainable intervention for various settings, from clinical rehabilitation to school physical education programs.
Despite these promising findings, several limitations must be acknowledged. The exclusive focus on male participants limits the generalizability of our findings to females with ADHD. Furthermore, the absence of follow-up assessments prevents conclusions about the long-term maintenance of acquired motor skills. Most notably, we did not measure potential changes in cognitive functions or ADHD core symptoms despite table tennis's documented benefits for executive functions, preventing examination of whether motor improvements translated into broader functional gains. Additionally, the remarkably large effect sizes should be interpreted cautiously within our specific methodological context.
Future research should therefore investigate table tennis training in larger, more diverse samples including female participants, incorporate comprehensive assessment batteries measuring cognitive functions and ADHD symptom severity, and implement longitudinal designs with follow-up assessments. Building on previous methodology, researchers could adapt protocols from Tsai, Wang, and Tseng (27) and Jalilvand and Azadian (29) while addressing the identified limitations. Studies should also explore transfer effects to academic performance and social functioning, and investigate optimal training parameters for different ADHD presentations.
Conclusion
This study provides compelling evidence that structured table tennis training effectively improves fundamental motor skills in children with ADHD, with particularly strong effects on locomotor abilities. The differential impact across motor domains, high adherence rates, and multi-system benefits support integrating targeted racket sports into comprehensive treatment approaches. Based on our findings and consistent with previous research, we recommend that clinicians, educators, and parents consider incorporating table tennis into regular activity routines while researchers continue to explore the optimal parameters and broader benefits of such interventions.
Acknowledgement
The author sincerely appreciates the valuable assistance and support of all individuals who contributed to this research.
Funding sources
This research received no specific grant from any funding agency in the public, commercial, or not-for-profit sectors.
Ethical statement
This study was conducted in accordance with the ethical principles outlined in the Declaration of Helsinki. Ethical approval was granted by the Islamic Azad University Human Research Ethics Committee (Approval code: IR.IAU.H.REC.1403.039).
Conflicts of interest
The author declares no conflict of interest.
Author contributions
The author was solely responsible for all aspects of the study, including conception, design, data collection, analysis, and manuscript preparation.
Data availability statement
The data that support the findings of this study are available from the corresponding author upon reasonable request.
Editorial: Original article |
Subject:
Health
Received: 2025/08/20 | Accepted: 2025/09/25 | Published: 2025/09/30
Received: 2025/08/20 | Accepted: 2025/09/25 | Published: 2025/09/30
References
1. Jalilvand M, Samad H. The effectiveness of physical activity with motor-cognitive approach on executive function in children with Attention Deficit/Hyperactivity Disorder. Jorjani Biomed J. 2020;8(2):17-26. [View at Publisher] [DOI] [Google Scholar]
2. Liu HLV, Sun F, Anderson DI, Tse CYA. The effect of physical activity intervention on motor proficiency in children and adolescents with ADHD: A systematic review and meta-analysis. Child Psychiatry Hum Dev. 2025;56(1):177-91. [View at Publisher] [DOI] [PMID] [Google Scholar]
3. Gholamhoseini H, Jalilvand M. The Effect of Fundamental Motor Games on Motor Competence in Hyperactive Children. Shefaye Khatam. 2025;13(2):1-10. [View at Publisher] [DOI] [Google Scholar]
4. Kao P-H, Ho C-H, Huang CL-C. Sex differences in psychiatric comorbidities of attention-deficit/hyperactivity disorder among children, adolescents, and adults: A nationwide population-based cohort study. PLoS ONE. 2025;20(1):e0315587. [View at Publisher] [DOI] [PMID] [Google Scholar]
5. Kadri A, Slimani M, Bragazzi NL, Tod D, Azaiez F. Effect of taekwondo practice on cognitive function in adolescents with attention deficit hyperactivity disorder. Int J Environ Res Public Health. 2019;16(2):204. [View at Publisher] [DOI] [PMID] [Google Scholar]
6. Scott H, Shoulberg EK, Dennis M, Krasner A, Smith AL, Hoza B. Associations of ADHD-risk and motor competence with school functioning. J Atten Disord. 2024;28(1):31-42. [View at Publisher] [DOI] [PMID] [Google Scholar]
7. Kleeren L, Hallemans A, Hoskens J, Klingels K, Smits-Engelsman B, Verbecque E. A critical view on motor-based interventions to improve motor skill performance in children with ADHD: A systematic review and meta-analysis. J Atten Disord. 2023;27(4):354-67. [View at Publisher] [DOI] [PMID] [Google Scholar]
8. Jalilvand M, Souri R. The Effectiveness of Motor Activity-Based Executive Function Training on Working Memory and Sustained Attention of Children with Attention Deficit / Hyperactivity Disorder. Adv Cogn Sci. 2021;22(4):87-98. [View at Publisher] [DOI] [Google Scholar]
9. Roshan S, Souri R, Jalilvand M. Effectiveness of a Kata Exercise Course on Static and Dynamic Balance in Hyperactive Children. J Sport Biomech. 2024;9(4):272-83. [View at Publisher] [DOI] [Google Scholar]
10. Kuo H-I, Nitsche MA, Wu Y-T, Chang J-C, Yang L-K. Acute aerobic exercise modulates cognition and cortical excitability in adults with attention-deficit hyperactivity disorder (ADHD) and healthy controls. Psychiatry Res. 2024;340:116108. [View at Publisher] [DOI] [PMID] [Google Scholar]
11. Cortese S, Adamo N, Del Giovane C, Mohr-Jensen C, Hayes AJ, Carucci S, et al. Comparative efficacy and tolerability of medications for attention-deficit hyperactivity disorder in children, adolescents, and adults: A systematic review and network meta-analysis. Lancet Psychiatry. 2018;5(9):727-38. [View at Publisher] [DOI] [PMID] [Google Scholar]
12. Ludyga S, Hanke M, Leuenberger R, Bruggisser F, Pühse U, Gerber M, et al. Martial Arts and Cognitive Control in Children with Attention-Deficit Hyperactivity Disorder and Children Born Very Preterm: A Combined Analysis of two Randomized Controlled Trials. Med Sci Sports Exerc. 2023;55(5):777-86. [View at Publisher] [DOI] [PMID] [Google Scholar]
13. Zhao M, Hou M, Herold F, Chen Y, Werneck AO, Block ME, et al. Associations of meeting 24-hour movement behavior guidelines with social and emotional function in youth with ASD/ADHD. J Affect Disord. 2024; 359:189-95. [View at Publisher] [DOI] [PMID] [Google Scholar]
14. Song Y, Jia S, Wang X, Wang A, Ma T, Li S, et al. Effects of physical exercise on anxiety depression and emotion regulation in children with attention deficit hyperactivity disorder: A systematic review and meta-analysis. Front Pediatr. 2025;12:1479615. [View at Publisher] [DOI] [PMID] [Google Scholar]
15. Chan Y-S, Jang J-T, Ho C-S. Effects of physical exercise on children with attention deficit hyperactivity disorder. Biomed J. 2022;45(2):265-70. [View at Publisher] [DOI] [PMID] [Google Scholar]
16. Dewi R, Verawati I, Sukamton A, Hakim H, Burhaein E, Lourenço CCV. The Impact of Basic Motion Activities on Social Interaction in Elementary School Students. J Hum Mov Sport Sci. 2023;11(1):143-51. [View at Publisher] [DOI] [Google Scholar]
17. Lee J, Zhang T, Chu TLA, Gu X, Zhu P. Effects of a fundamental motor skill-based afterschool program on children's physical and cognitive health outcomes. Int J Environ Res Public Health. 2020;17(3):733. [View at Publisher] [DOI] [PMID] [Google Scholar]
18. Lowe CT, Curry CJ, Climie EA, Jiang Y, Rogers MA, Corkum P, et al. Navigating prolonged stressor events: Exploring the unexpected relationship with mental health and physical activity in children with attention-deficit/hyperactivity disorder. Neurodiversity. 2025;3:27546330241301932. [View at Publisher] [DOI] [Google Scholar]
19. NajafiShahna M, Dinan PH, Ahmadpour A. The Effect of Fundamental Motor Skill Training by "Teaching Game for Understanding" Approach on Motor and Cognitive Skills in Children With Attention-Deficit/Hyperactivity Disorder. Sci J Rehabil Med. 2024;13(2):392-405. [View at Publisher] [DOI] [Google Scholar]
20. Rasoolyar Z, Jalilvand M. Effectiveness of Yoga Exercises on Static and Dynamic Balance in Children with Attention Deficit/Hyperactivity Disorder. Sci J Rehabil Med. 2021;9(4):278-88. [View at Publisher] [DOI] [Google Scholar]
21. Feng L, Li B, Yong SS, Tian Z. Effects of exercise intervention on physical and mental health of children and adolescents with attention-deficit/hyperactivity disorder: A systematic review and meta-analysis based on ICF-CY. J Sci Sport Exerc. 2024;8:1-8. [View at Publisher] [DOI] [Google Scholar]
22. González-Devesa D, Sanchez-Lastra MA, Pintos-Barreiro M, Ayán-Pérez C. Benefits of table tennis for children and adolescents: A narrative review. Children. 2024;11(8):963. [View at Publisher] [DOI] [PMID] [Google Scholar]
23. Chagas DV, Macedo LP, Batista LA. The effect of one year of unstructured table tennis participation on motor coordination level among young recreational players. Arch Med Deporte. 2018;35(186):223-7. [View at Publisher] [Google Scholar]
24. Pan C-Y, Tsai C-L, Chu C-H, Sung M-C, Huang C-Y, Ma W-Y. Effects of physical exercise intervention on motor skills and executive functions in children with ADHD: A pilot study. J Atten Disord. 2019;23(4):384-97. [View at Publisher] [DOI] [PMID] [Google Scholar]
25. Basiri F, Farsi A, Abdoli B, Kavyani M. The Effect of Visual and Tennis Training on Perceptual-Motor Skill and Learning of Forehand Drive in Table Tennis Players. J Mod Rehabil. 2020;14(1):21-32. [View at Publisher] [DOI] [Google Scholar]
26. Qiu C, Zhai Q, Chen S. Effects of Practicing Closed-vs. Open-Skill Exercises on Executive Functions in Individuals with Attention Deficit Hyperactivity Disorder (ADHD)-A Meta-Analysis and Systematic Review. Behav Sci. 2024;14(6):499. [View at Publisher] [DOI] [PMID] [Google Scholar]
27. Tsai C-L, Wang C-H, Tseng Y-T. Effects of exercise intervention on event-related potential and task performance indices of attention networks in children with developmental coordination disorder. Brain Cogn. 2012;79(1):12-22. [View at Publisher] [DOI] [PMID] [Google Scholar]
28. Jalilvand M. Effectiveness of Yoga and Table Tennis Exercises on Static and Dynamic Balance of Deaf Children: The Role of Balance Sensory Receptors and Neural Mechanisms of Open and Closed-Loop Control. Neurosci J Shefaye Khatam. 2021;10(1):75-84. [View at Publisher] [DOI] [Google Scholar]
29. Jalilvand M, Azadian E. The effectiveness of open and closed loop control exercises on static and dynamic balance in children with attention deficit hyperactivity disorder. Mind Mov Behav. 2022;1(1):121-35. [View at Publisher] [DOI] [Google Scholar]
30. Bahram ME, Assarian F, Atoof F, Taghadosi M, Akkasheh N, Akkasheh G. Effect of a 12-week interval running program on female primary school students with ADHD. Feyz. Feyz Med Sci J. 2014;18(2):151-8. [View at Publisher] [Google Scholar]
31. Bakhshipour E, Rahnama N, Sourtiji H, Skandari Z, Izadi Najafabadi S. Comparing the effects of an aerobic exercise program and group-based play therapy on the balance of children with Attention Deficit Hyperactive Disorder (ADHD). J Res Rehabil Sci. 2013;9(2):161-70. [View at Publisher] [DOI] [Google Scholar]
32. Eskandarnejad M, Jahedi Khajeh M, Rezaee F. Impact of Perceptual-Motor Training Basketball on Balance Function of Children with Attention Deficit Hyperactivity Disorder. Sci J Rehabil Med. 2017;6(3):135-43. [View at Publisher] [DOI] [Google Scholar]
33. Keykhahosseinpoor A, Rahnama N, Skandary Z. Comparison of the Effect of Aerobic Exercise and Group Play Therapy on the Coordination and Agility Skills in Children with Attention Deficit Hyperactivity Disorder. J Paramed Sci Rehabil. 2020;9(3):7-18. [View at Publisher] [DOI] [Google Scholar]
34. Liang X, Qiu H, Tsai C-L, Li C, Sit CH. MVPA and Motor Proficiency between Children with ADHD and Typical Development: Associations with Sleep Quality. Med Sci Sports Exerc. 2023;55(10):1886-93. [View at Publisher] [DOI] [PMID] [Google Scholar]
35. Gu Y, Yu C, Shao S, Baker JS. Effects of table tennis multi-ball training on dynamic posture control. PeerJ. 2019;6:e6262. [View at Publisher] [DOI] [PMID] [Google Scholar]
36. Tas M, Sinanoglu A. Effect of Table Tennis Trainings on Certain Physical and Physiological Parameters in Children Aged 10-12. J Educ Train Stud. 2017;5(3):11-9. [View at Publisher] [DOI] [Google Scholar]
37. Chen M-D, Tsai H-Y, Wang C-C, Wuang Y-P. The effectiveness of racket-sport intervention on visual perception and executive functions in children with mild intellectual disabilities and borderline intellectual functioning. Neuropsychiatr Dis Treat. 2015;11:2287-97. [View at Publisher] [DOI] [PMID] [Google Scholar]
38. Pan C-Y, Chu C-H, Tsai C-L, Lo S-Y, Cheng Y-W, Liu Y-J. A racket-sport intervention improves behavioral and cognitive performance in children with attention-deficit/hyperactivity disorder. Res Dev Disabil. 2016;57:1-10. [View at Publisher] [DOI] [PMID] [Google Scholar]
39. Moreau D, Morrison AB, Conway AR. An ecological approach to cognitive enhancement: Complex motor training. Acta Psychol. 2015;157:44-55. [View at Publisher] [DOI] [PMID] [Google Scholar]
40. Visser A, Büchel D, Lehmann T, Baumeister J. Continuous table tennis is associated with processing in frontal brain areas: An EEG approach. Exp Brain Res. 2022;240(6):1899-909. [View at Publisher] [DOI] [PMID] [Google Scholar]
Send email to the article author
| Rights and permissions | |
 |
This work is licensed under a Creative Commons Attribution-NonCommercial 4.0 International License. |
