
Volume 13, Issue 3 (10-2025)
Jorjani Biomed J 2025, 13(3): 31-36 |
Back to browse issues page


Download citation:
BibTeX | RIS | EndNote | Medlars | ProCite | Reference Manager | RefWorks
Send citation to:



BibTeX | RIS | EndNote | Medlars | ProCite | Reference Manager | RefWorks
Send citation to:
Alishahi V, Alishahi A. Side-specific pain responses to cosmetic botulinum toxin type A injections in 5 Azar Hospital and a private clinic in Gorgan in 2025 year: A cross-sectional study of the forehead. Jorjani Biomed J 2025; 13 (3) :31-36
URL: http://goums.ac.ir/jorjanijournal/article-1-1096-en.html
URL: http://goums.ac.ir/jorjanijournal/article-1-1096-en.html



1- Department of Surgery, Clinical Research Development Unit (CRDU), Golestan University of Medical Sciences, Gorgan, Iran
2- Department of Surgery, Golestan University of Medical Sciences, Gorgan, Iran ,ali1000alishah@gmail.com
2- Department of Surgery, Golestan University of Medical Sciences, Gorgan, Iran ,
Full-Text [PDF 500 kb]
(473 Downloads)
| Abstract (HTML) (3182 Views)
Discussion
Gender and age
Significant statistical differences in pain scores were found between female and male participants on both sides. In accordance with the present results, this finding is particularly noteworthy, as it diverges from the broader pain literature, which often reports greater pain sensitivity or prevalence in females across various noxious stimuli (5). In a study conducted by Molaei et al., the response to botulinum toxin type A therapy in patients with treatment-resistant migraine headaches showed that the reduction in the incidence of migraine episodes in men was significantly greater than in women over time (12).
In Aoki’s investigation, the evidence indicates that chronic migraine - one of the primary indications for botulinum toxin therapy - is significantly more prevalent in women than in men. This gender disparity is reflected in the patient populations of clinical trials, which predominantly consist of women. Furthermore, the article suggests that gonadal hormones, particularly estrogen, may influence susceptibility to chronic pain conditions and potentially modulate the response to botulinum toxin treatment (13). Dima et al. reported that Botox is a highly effective prophylactic (Preventive) treatment for chronic migraine, with significant benefit demonstrated predominantly in women, as they comprise the majority of the affected patient population and clinical trial participants due to the higher prevalence of chronic migraine in females (14).
In our survey, age did not have a statistically significant relationship with pain caused by Botox injection. Consistent with this result, Turner-Stokes et al. (2025) found that age did not significantly influence the reduction in pain scores following BoNT-A injections. Both younger and older patients experienced similar levels of pain relief, indicating that age is not a determining factor in treatment outcomes (15). Atraszkiewicz’s study found that female gender and adult age are two main demographic factors that place an individual at risk of developing chronic migraine (16).
Bravo et al. (2021), in their study "Individualizing BoNT-A Doses According to Age," reported that dosing requirements are negatively correlated with age, except in the periorbital area, where an increase in dose was observed. This suggests that older patients may require different dosing strategies, which could influence pain perception (17). Santana et al. (2021), in a study on BoNT-A injections in pediatric patients with chronic migraines (Ages 11-18), suggested that age may influence pain perception and tolerance during injections (18). Additionally, Kahn et al. (2018), examining BoNT-A for myofascial pain in temporomandibular joint disorders, found that age may impact injection effectiveness - possibly due to age-related differences in pain perception and treatment response (19).
The divergence of our findings from previous literature may stem from differences in injection region, sample composition, and methodological controls. The predominance of young female participants in our study, as well as cultural and psychological differences in pain reporting, may have influenced subjective pain scores. Moreover, forehead injections involve distinct sensory innervation and skin thickness compared to other facial or cervical areas examined in prior studies, potentially explaining the observed gender-related variation.
Body mass index
At present, a significant relationship was found between BMI and pain. In line with our findings, Wu-Fienberg et al. (2018) reported that as BMI increases, the distance between the skin surface and the underlying muscle fascia increases, which may affect the depth of injection and potentially influence pain perception during the procedure (20). On the other hand, a study that compared the incidence and characteristics of neck pain in patients receiving BoNT-A injections using different needle lengths showed that BMI did not significantly correlate with the incidence or characteristics of neck pain, suggesting that BMI may not be a major factor influencing pain perception during BoNT-A injections (21). This inconsistency across studies may be attributed to anatomical differences in injection sites, since subcutaneous fat distribution in the forehead differs from that of the neck or trunk. In our sample, participants with higher BMI likely experienced greater needle pressure or tissue resistance, intensifying pain perception. Additionally, localized edema and variations in vascularity may further modulate nociceptive responses, contributing to these differences.
Handedness
Bivariate correlations revealed a non-significant relationship between left- and right-side pain scores, indicating a general consistency in pain reporting across both sides of the forehead. In a larger study, Fouché et al. (2017) investigated pain asymmetry in 302 patients receiving botulinum toxin or soft tissue filler injections and found consistently greater discomfort on the left side, particularly among right-handed individuals (4). In a sample of 351 healthy individuals subjected to unpleasant heat stimulation on both hands, Lugo et al. found that pain ratings on a Visual Analog Scale (VAS) were significantly higher on the left hand compared to the right, suggesting right hemisphere dominance in pain processing (22). In cosmetic injections, mechanical and psychological factors such as anticipation of pain or practitioner hand dominance may influence perceived asymmetry. The subtle lateralized trend observed in our data could thus reflect both neurophysiological and procedural elements unique to aesthetic injections.
Needle size
In the present study, no significant statistical relationship was found between injection pain and needle size. In contrast, Alam et al. (2015) evaluated the effect of needle gauge on pain during botulinum toxin injections and found that 30-gauge needles caused more pain than 32-gauge needles (23). Kämmerer et al. (2024), in a study comparing pain perception during BoNT-A injections using 30G, 33G, and 34G needles in the head and neck region, indicated that patients reported less discomfort with 33G and 34G needles compared to 30G needles, with 34G needles causing the least discomfort. In fact, smaller gauge needles (33G and 34G) are associated with reduced pain perception during BoNT-A injections (24). Maytharakcheep et al. (2024) also reported that micro-hypodermic needles resulted in reduced pain and bruising compared to standard needles, while maintaining similar therapeutic efficacy (25).
The lack of association in our results may be due to the relatively uniform needle sizes used in this study, where most injections were performed with 33G needles, limiting comparative variability. Furthermore, patient factors such as anxiety or injection speed could have outweighed the minor mechanical differences between gauges, leading to non-significant findings. Abreu Venancio et al. showed that the use of a finer-gauge needle (A thinner needle) is associated with reduced tissue trauma, pain, and bleeding at the injection site. This, in turn, can lead to a lower incidence and severity of short-term, procedure-related headaches following the injection (26).
History of injection
At present, it is noteworthy that the number of prior injection sessions showed a statistical trend toward reducing pain asymmetry. However, the borderline significance of this finding necessitates caution in its interpretation and underscores the need for verification in larger cohorts. In a study conducted by Shymaa et al. (2019), prior exposure to botulinum toxin injections was associated with lower perceived pain intensity, suggesting a possible adaptation or desensitization effect that could influence patient comfort in therapeutic settings such as carpal tunnel treatment (27). In a systematic review of patient outcomes across both aesthetic and therapeutic settings, Meretsky et al. (2024) highlighted improved quality of life and high satisfaction rates following BoNT-A treatment, findings that align with the positive functional outcomes observed in our cohort (28). Turner-Stokes et al. (2025) found no significant correlation between a patient's history of prior BoNT-A injections and the reduction in pain scores. However, patients requiring more frequent injections tended to have higher baseline pain scores and a smaller reduction in pain scores over time (15).
Other factors, such as the professional skill of the physician, may also affect pain. Borba et al. (2022) examined the adverse effects of botulinum toxin injections and determined that complications are minimal when administered by proficient practitioners (29). Although their investigation focused on safety outcomes rather than discomfort, Kaplan et al. (2017) emphasized the necessity of a precise anatomical understanding of facial musculature to achieve optimal cosmetic results (30). Although their research did not directly address pain, it supports the idea that anatomical variations influence patient experiences, underscoring the importance of skilled practitioners and individualized treatment approaches.
In our population, individuals with repeated exposure likely developed psychological tolerance and reduced anxiety, decreasing perceived pain. Furthermore, consistent administration by a single experienced physician may have standardized technique and minimized procedural variability, contributing to lower pain asymmetry among experienced participants. Indeed, in the present study, the borderline significance of this association should be interpreted with caution and requires validation in larger studies.
Conclusion
Female participants and those with higher BMI reported greater discomfort, while previous injection experience appeared to mitigate pain asymmetry. These findings highlight the need for individualized injection strategies based on patient characteristics and anatomical variations to enhance comfort and satisfaction. Further research is recommended to clarify the underlying neurophysiological mechanisms of pain lateralization in aesthetic procedures.
Limitations
The sample was predominantly young, right-handed females, which may limit the generalizability of the findings to other populations. Second, all injections were performed by a single experienced physician, so the influence of operator variability on pain perception could not be assessed. Third, pain was measured immediately after injection using a subjective scale (VAS), which may be affected by individual perception and reporting bias. Finally, the cross-sectional design prevents assessment of long-term changes in pain perception or adaptation over multiple injection sessions. The sample size, while adequate for the primary paired analysis, limited the power for subgroup analyses (e.g., by gender, substance use). Findings from these exploratory subgroup comparisons should be interpreted with caution and require validation in larger, adequately powered studies.
Acknowledgement
The authors would like to express their gratitude to the nursing staff and administrators of the surgical department of 5 Azar Hospital and the private clinic in Gorgan for their invaluable cooperation and assistance in patient recruitment and data collection. We also extend our sincere thanks to all the participants who took part in this study.
Funding sources
This study is not supported/funded.
Ethical statement
The study protocol was approved by the Ethics Committee of Golestan University of Medical Sciences (No. IR.GOUMS.REC.1403.096). The study was conducted in accordance with the ethical standards of the institutional and national research committee and with the 1964 Helsinki Declaration and its later amendments.
Conflicts of interest
The manuscript has been read and approved by all authors. The authors affirm that the requirements for authorship have been met and that the manuscript represents honest and original work.
Author contributions
Valiollah Alishahi: Conceptualization, methodology, formal analysis, investigation, data curation, writing original draft, and project administration; Ali Alishahi: Methodology, validation, investigation, resources, writing review, editing, and supervision.
Data availability statement
The datasets generated and analyzed during the current study are not publicly available due to participant privacy considerations but are available from the corresponding author upon reasonable request.
Full-Text: (68 Views)
Introduction
Cosmetic procedures have gained significant popularity in recent years, with botulinum toxin (Botox) injections being one of the most common non-invasive methods for facial rejuvenation. The forehead is among the most frequently treated areas due to hyperactive frontalis muscles, which are a primary cause of dynamic wrinkles (1,2). Despite its widespread use, Botox is not without risks. These include diplopia, asymmetry, brow ptosis, and localized pain, complications often attributed to the complex and not yet fully elucidated anatomy of the forehead muscles (3). Interestingly, several studies have reported that individuals may experience varying degrees of pain on the right versus the left side of the body following cosmetic injections. For instance, Fouché et al. (2017) reported a statistically significant left-side dominance in pain during cosmetic facial injections, with a mean pain score of 3.31 on the left compared to 2.79 on the right (4). Also, Pud et al. (2009), applying thermal stimuli to the hands, found that pain ratings on a Visual Analog Scale (VAS) were significantly higher on the left hand compared to the right. A neurophysiological explanation for this lateralized sensory experience may lie in the predominant role of the right cerebral hemisphere in processing pain perception (5,6). Of the seven serotypes (A-G), types A and B are the most widely used in therapeutic practice, with type A being the standard in cosmetic applications (7).
Beyond aesthetics, botulinum toxin plays a critical role in managing a wide range of medical conditions, including strabismus, focal dystonias, hemifacial spasm, spastic movement disorders, headaches, hypersalivation, hyperhidrosis, and certain chronic disorders that respond only partially to conventional pharmacologic therapies. The list of potential new indications continues to expand rapidly (8). In cosmetic medicine, it is primarily used to soften dynamic wrinkles, especially in the forehead, glabella, and periorbital regions. Clinical effects typically begin 4 to 7 days after injection and last for 3 to 6 months (2).
Although generally well tolerated, Botox injections can cause temporary muscle paralysis, bruising, edema, and localized pain (9). Perception of this pain can be influenced by anatomical location, injection technique, and individual pain threshold (10). The evolving role of botulinum toxin in modern medicine is further reflected in its expanding indications, which now include chronic pain and psychiatric disorders (11).
This study aims to investigate potential differences in pain perception between the left and right sides of the forehead during cosmetic botulinum toxin injections. Understanding this asymmetry is essential for optimizing patient experience and tailoring procedural planning. Therefore, this cross-sectional study was conducted at 5 Azar Hospital and a private clinic in Gorgan, Iran.
Methods
Study design and setting
A cross-sectional study was conducted in the surgical department of the 5 Azar Educational and Therapeutic Hospital and in a private clinic in Gorgan city, Iran, between January and September 2024. The study population consisted of all individuals seeking cosmetic botulinum toxin type A injection for the forehead region during the specified study period. Prior to the study, written informed consent was obtained from all participants. The study protocol was approved by the Ethics Committee of Golestan University of Medical Sciences (Approval No. IR.GOUMS.REC.1403.096) and was conducted in accordance with the ethical standards of the institutional and/or national research committee and with the 1964 Helsinki Declaration and its later amendments.
Sample size calculation
According to a study by Fouché Jacobus et al. (2017), the average and standard deviation of pain scores on the right and left sides were 3.31 ± 1.73 and 2.79 ± 1.63, respectively. Using the paired sample formula and assuming a 95% confidence level and 80% statistical power, the required sample size was determined to be 84 participants in each group (i.e., per injection side), for a total of 168 (4).
Participants
Participants were eligible for inclusion if they were between 25 and 55 years old, were undergoing botulinum toxin injection for the first time or had not received it in the past year, and had no history of neurological, sensory, or motor disorders. Additionally, eligible participants reported normal cutaneous sensitivity to pressure, touch, and temperature. Individuals were excluded if they had a known hypersensitivity to botulinum toxin or any injection materials, presented with chronic skin conditions in the injection area, were pregnant or breastfeeding, or did not provide informed consent.
Procedure
All participants initially completed an intake form documenting demographic information, including age and gender, as well as any history of substance use (e.g., smoking, narcotics, hookah). A brief pain sensitivity assessment was then administered by a physician. During this test, patients were instructed to close their eyes while a cotton swab was gently stroked across each side of the face. Participants were also asked about any history of unilateral facial pain.
The botulinum toxin type A used was the brand Behnoodpharmed, a 500-unit vial. For each participant, a total of 4 units (2 units per side) was injected into the forehead. Approximately thirty 500-unit vials with different serial numbers and a uniform expiry date of 2025 were used, following the manufacturer’s recommended storage and reconstitution guidelines.
To minimize potential confounding variables, all injections were administered by a single subspecialty board-certified cosmetic and plastic surgeon. The initial side of injection was randomly assigned for each participant. This was systematically recorded using a numbering system in which odd-numbered participants received the first injection on the left side and even-numbered participants received the first injection on the right side. All procedural details were accurately documented in the participant questionnaire.
Outcome measurement
Pain intensity was self-reported by participants on a 10-cm Visual Analog Scale (VAS), where 0 indicated “no pain” and 10 indicated “worst possible pain.” Participants were instructed on the use of the scale prior to injection. Each participant was instructed to rate their perceived level of pain five minutes following the injection procedure. All responses were meticulously documented using a standardized pain evaluation form to ensure consistent data collection (1).
Allocation concealment and blinding
The numbering was based on the sequential order of patient enrollment. The physician was unaware of the next participant’s number until after they were formally enrolled. While the injecting physician could not be blinded to the injection side, the key outcome assessor (The patient) was blinded to the specific hypothesis regarding side-specific pain differences. Patients were not informed that the study was investigating left–right asymmetry, reducing the likelihood of reporting bias. The fact that every participant served as their own control (Paired design) and that a single, experienced physician performed all injections using a standardized technique helps minimize the potential impact of quasi-randomization on the core finding of side-specific pain differences.
Statistical analysis
Descriptive statistics, including mean and standard deviation for continuous variables and frequency and percentage for categorical variables, were used to summarize the data. The normality of the distribution of pain score differences (VAS) between the left and right sides was assessed for the entire cohort and within subgroups (e.g., gender, age group, BMI, history of substance use) using the Shapiro-Wilk and Kolmogorov-Smirnov tests and visual inspection of Q-Q plots.
For the primary analysis comparing pain between the left and right forehead within the same individuals, a paired t-test was used. Independent t-tests were employed to compare mean pain scores between demographic subgroups such as gender (Male vs. female) and addiction status (Yes vs. no). The relationships between continuous variables such as age, BMI, and number of prior injections with pain scores were assessed using Pearson correlation.
Finally, a multiple linear regression model was performed to identify significant predictors (e.g., sex, BMI, prior injections) of the pain difference between sides. All critical assumptions for the multiple regression model were verified. The Variance Inflation Factor (VIF) confirmed the absence of multicollinearity, with all values below 5. Diagnostic plots demonstrated linear relationships and homoscedasticity of residuals. Furthermore, a Q-Q plot and the Shapiro-Wilk test confirmed that residuals did not significantly deviate from a normal distribution, validating the model’s appropriateness. A p-value of less than 0.05 was considered statistically significant for all analyses. All statistical analyses were performed using SPSS software (Version 16).
Results
A total of 84 participants were included in the analysis, of whom 81% were female and 91.7% were right-handed. Most injections (67.9%) were performed using 33-gauge needles, and the majority of participants (83.3%) reported no history of substance use. Approximately one-fifth (17.9%) had never undergone Botox injections before, while others reported between one and four prior sessions. These demographic data demonstrate a sample predominantly composed of young, right-handed females with prior exposure to cosmetic procedures (Table 1).
Cosmetic procedures have gained significant popularity in recent years, with botulinum toxin (Botox) injections being one of the most common non-invasive methods for facial rejuvenation. The forehead is among the most frequently treated areas due to hyperactive frontalis muscles, which are a primary cause of dynamic wrinkles (1,2). Despite its widespread use, Botox is not without risks. These include diplopia, asymmetry, brow ptosis, and localized pain, complications often attributed to the complex and not yet fully elucidated anatomy of the forehead muscles (3). Interestingly, several studies have reported that individuals may experience varying degrees of pain on the right versus the left side of the body following cosmetic injections. For instance, Fouché et al. (2017) reported a statistically significant left-side dominance in pain during cosmetic facial injections, with a mean pain score of 3.31 on the left compared to 2.79 on the right (4). Also, Pud et al. (2009), applying thermal stimuli to the hands, found that pain ratings on a Visual Analog Scale (VAS) were significantly higher on the left hand compared to the right. A neurophysiological explanation for this lateralized sensory experience may lie in the predominant role of the right cerebral hemisphere in processing pain perception (5,6). Of the seven serotypes (A-G), types A and B are the most widely used in therapeutic practice, with type A being the standard in cosmetic applications (7).
Beyond aesthetics, botulinum toxin plays a critical role in managing a wide range of medical conditions, including strabismus, focal dystonias, hemifacial spasm, spastic movement disorders, headaches, hypersalivation, hyperhidrosis, and certain chronic disorders that respond only partially to conventional pharmacologic therapies. The list of potential new indications continues to expand rapidly (8). In cosmetic medicine, it is primarily used to soften dynamic wrinkles, especially in the forehead, glabella, and periorbital regions. Clinical effects typically begin 4 to 7 days after injection and last for 3 to 6 months (2).
Although generally well tolerated, Botox injections can cause temporary muscle paralysis, bruising, edema, and localized pain (9). Perception of this pain can be influenced by anatomical location, injection technique, and individual pain threshold (10). The evolving role of botulinum toxin in modern medicine is further reflected in its expanding indications, which now include chronic pain and psychiatric disorders (11).
This study aims to investigate potential differences in pain perception between the left and right sides of the forehead during cosmetic botulinum toxin injections. Understanding this asymmetry is essential for optimizing patient experience and tailoring procedural planning. Therefore, this cross-sectional study was conducted at 5 Azar Hospital and a private clinic in Gorgan, Iran.
Methods
Study design and setting
A cross-sectional study was conducted in the surgical department of the 5 Azar Educational and Therapeutic Hospital and in a private clinic in Gorgan city, Iran, between January and September 2024. The study population consisted of all individuals seeking cosmetic botulinum toxin type A injection for the forehead region during the specified study period. Prior to the study, written informed consent was obtained from all participants. The study protocol was approved by the Ethics Committee of Golestan University of Medical Sciences (Approval No. IR.GOUMS.REC.1403.096) and was conducted in accordance with the ethical standards of the institutional and/or national research committee and with the 1964 Helsinki Declaration and its later amendments.
Sample size calculation
According to a study by Fouché Jacobus et al. (2017), the average and standard deviation of pain scores on the right and left sides were 3.31 ± 1.73 and 2.79 ± 1.63, respectively. Using the paired sample formula and assuming a 95% confidence level and 80% statistical power, the required sample size was determined to be 84 participants in each group (i.e., per injection side), for a total of 168 (4).
Participants
Participants were eligible for inclusion if they were between 25 and 55 years old, were undergoing botulinum toxin injection for the first time or had not received it in the past year, and had no history of neurological, sensory, or motor disorders. Additionally, eligible participants reported normal cutaneous sensitivity to pressure, touch, and temperature. Individuals were excluded if they had a known hypersensitivity to botulinum toxin or any injection materials, presented with chronic skin conditions in the injection area, were pregnant or breastfeeding, or did not provide informed consent.
Procedure
All participants initially completed an intake form documenting demographic information, including age and gender, as well as any history of substance use (e.g., smoking, narcotics, hookah). A brief pain sensitivity assessment was then administered by a physician. During this test, patients were instructed to close their eyes while a cotton swab was gently stroked across each side of the face. Participants were also asked about any history of unilateral facial pain.
The botulinum toxin type A used was the brand Behnoodpharmed, a 500-unit vial. For each participant, a total of 4 units (2 units per side) was injected into the forehead. Approximately thirty 500-unit vials with different serial numbers and a uniform expiry date of 2025 were used, following the manufacturer’s recommended storage and reconstitution guidelines.
To minimize potential confounding variables, all injections were administered by a single subspecialty board-certified cosmetic and plastic surgeon. The initial side of injection was randomly assigned for each participant. This was systematically recorded using a numbering system in which odd-numbered participants received the first injection on the left side and even-numbered participants received the first injection on the right side. All procedural details were accurately documented in the participant questionnaire.
Outcome measurement
Pain intensity was self-reported by participants on a 10-cm Visual Analog Scale (VAS), where 0 indicated “no pain” and 10 indicated “worst possible pain.” Participants were instructed on the use of the scale prior to injection. Each participant was instructed to rate their perceived level of pain five minutes following the injection procedure. All responses were meticulously documented using a standardized pain evaluation form to ensure consistent data collection (1).
Allocation concealment and blinding
The numbering was based on the sequential order of patient enrollment. The physician was unaware of the next participant’s number until after they were formally enrolled. While the injecting physician could not be blinded to the injection side, the key outcome assessor (The patient) was blinded to the specific hypothesis regarding side-specific pain differences. Patients were not informed that the study was investigating left–right asymmetry, reducing the likelihood of reporting bias. The fact that every participant served as their own control (Paired design) and that a single, experienced physician performed all injections using a standardized technique helps minimize the potential impact of quasi-randomization on the core finding of side-specific pain differences.
Statistical analysis
Descriptive statistics, including mean and standard deviation for continuous variables and frequency and percentage for categorical variables, were used to summarize the data. The normality of the distribution of pain score differences (VAS) between the left and right sides was assessed for the entire cohort and within subgroups (e.g., gender, age group, BMI, history of substance use) using the Shapiro-Wilk and Kolmogorov-Smirnov tests and visual inspection of Q-Q plots.
For the primary analysis comparing pain between the left and right forehead within the same individuals, a paired t-test was used. Independent t-tests were employed to compare mean pain scores between demographic subgroups such as gender (Male vs. female) and addiction status (Yes vs. no). The relationships between continuous variables such as age, BMI, and number of prior injections with pain scores were assessed using Pearson correlation.
Finally, a multiple linear regression model was performed to identify significant predictors (e.g., sex, BMI, prior injections) of the pain difference between sides. All critical assumptions for the multiple regression model were verified. The Variance Inflation Factor (VIF) confirmed the absence of multicollinearity, with all values below 5. Diagnostic plots demonstrated linear relationships and homoscedasticity of residuals. Furthermore, a Q-Q plot and the Shapiro-Wilk test confirmed that residuals did not significantly deviate from a normal distribution, validating the model’s appropriateness. A p-value of less than 0.05 was considered statistically significant for all analyses. All statistical analyses were performed using SPSS software (Version 16).
Results
A total of 84 participants were included in the analysis, of whom 81% were female and 91.7% were right-handed. Most injections (67.9%) were performed using 33-gauge needles, and the majority of participants (83.3%) reported no history of substance use. Approximately one-fifth (17.9%) had never undergone Botox injections before, while others reported between one and four prior sessions. These demographic data demonstrate a sample predominantly composed of young, right-handed females with prior exposure to cosmetic procedures (Table 1).
|
|
 Table 1. Sociodemographic and clinical profile of the sample |
Bivariate correlations revealed a non-significant relationship between left- and right-side pain scores (R = 0.210, P-Value = 0.056), indicating a general consistency in pain reporting across both sides of the forehead. A significant negative correlation was found between the number of previous Botox sessions and the mean pain difference (R = -0.227, P-Value = 0.038), suggesting that greater injection experience was associated with reduced pain asymmetry. No meaningful associations were observed between pain intensity and age or needle size. Overall, demographic factors demonstrated limited predictive value for explaining variations in pain perception (Table 2).
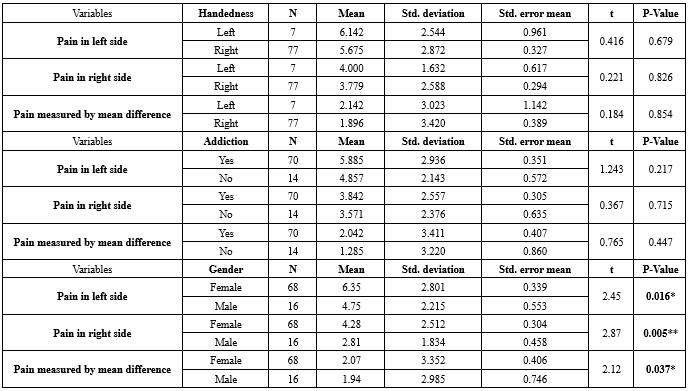
When stratified by handedness, addiction, and gender, pain perception remained higher on the left side for nearly all subgroups. Female participants reported significantly higher mean pain scores than males on both sides (P-Value = 0.037), particularly on the left. Right-handed participants also exhibited slightly higher pain on the left side, though this difference was not statistically significant. Addiction status showed minimal influence on pain levels. Collectively, these findings suggest a subtle but consistent lateralized pattern of pain, with greater discomfort on the left forehead (Table 3).
The multiple linear regression model confirmed these trends. The model was significant and accounted for 8.6% of the variance in the pain difference between sides (R² = 0.086). Among all tested predictors, sex (P-Value = 0.025) and BMI (P-Value = 0.012) were significantly associated with pain difference, while the number of previous Botox sessions suggested a trend toward reduced pain asymmetry (P-Value = 0.050). Other variables, including age, needle size, handedness, and addiction, were not significant contributors. The model explained a modest proportion of the variance in pain asymmetry, implying that neurophysiological or perceptual factors beyond demographic characteristics may play a larger role in shaping pain experiences during botulinum toxin injection (Table 4).
When stratified by handedness, addiction, and gender, pain perception remained higher on the left side for nearly all subgroups. Female participants reported significantly higher mean pain scores than males on both sides (P-Value = 0.037), particularly on the left. Right-handed participants also exhibited slightly higher pain on the left side, though this difference was not statistically significant. Addiction status showed minimal influence on pain levels. Collectively, these findings suggest a subtle but consistent lateralized pattern of pain, with greater discomfort on the left forehead (Table 3).
The multiple linear regression model confirmed these trends. The model was significant and accounted for 8.6% of the variance in the pain difference between sides (R² = 0.086). Among all tested predictors, sex (P-Value = 0.025) and BMI (P-Value = 0.012) were significantly associated with pain difference, while the number of previous Botox sessions suggested a trend toward reduced pain asymmetry (P-Value = 0.050). Other variables, including age, needle size, handedness, and addiction, were not significant contributors. The model explained a modest proportion of the variance in pain asymmetry, implying that neurophysiological or perceptual factors beyond demographic characteristics may play a larger role in shaping pain experiences during botulinum toxin injection (Table 4).

|
Table 4. Unstandardized and standardized coefficients for regression of pain difference on patient characteristics
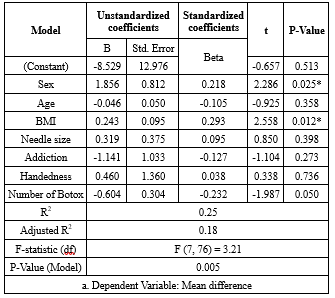 *Significant correlation: P < 0.05 |
Discussion
Gender and age
Significant statistical differences in pain scores were found between female and male participants on both sides. In accordance with the present results, this finding is particularly noteworthy, as it diverges from the broader pain literature, which often reports greater pain sensitivity or prevalence in females across various noxious stimuli (5). In a study conducted by Molaei et al., the response to botulinum toxin type A therapy in patients with treatment-resistant migraine headaches showed that the reduction in the incidence of migraine episodes in men was significantly greater than in women over time (12).
In Aoki’s investigation, the evidence indicates that chronic migraine - one of the primary indications for botulinum toxin therapy - is significantly more prevalent in women than in men. This gender disparity is reflected in the patient populations of clinical trials, which predominantly consist of women. Furthermore, the article suggests that gonadal hormones, particularly estrogen, may influence susceptibility to chronic pain conditions and potentially modulate the response to botulinum toxin treatment (13). Dima et al. reported that Botox is a highly effective prophylactic (Preventive) treatment for chronic migraine, with significant benefit demonstrated predominantly in women, as they comprise the majority of the affected patient population and clinical trial participants due to the higher prevalence of chronic migraine in females (14).
In our survey, age did not have a statistically significant relationship with pain caused by Botox injection. Consistent with this result, Turner-Stokes et al. (2025) found that age did not significantly influence the reduction in pain scores following BoNT-A injections. Both younger and older patients experienced similar levels of pain relief, indicating that age is not a determining factor in treatment outcomes (15). Atraszkiewicz’s study found that female gender and adult age are two main demographic factors that place an individual at risk of developing chronic migraine (16).
Bravo et al. (2021), in their study "Individualizing BoNT-A Doses According to Age," reported that dosing requirements are negatively correlated with age, except in the periorbital area, where an increase in dose was observed. This suggests that older patients may require different dosing strategies, which could influence pain perception (17). Santana et al. (2021), in a study on BoNT-A injections in pediatric patients with chronic migraines (Ages 11-18), suggested that age may influence pain perception and tolerance during injections (18). Additionally, Kahn et al. (2018), examining BoNT-A for myofascial pain in temporomandibular joint disorders, found that age may impact injection effectiveness - possibly due to age-related differences in pain perception and treatment response (19).
The divergence of our findings from previous literature may stem from differences in injection region, sample composition, and methodological controls. The predominance of young female participants in our study, as well as cultural and psychological differences in pain reporting, may have influenced subjective pain scores. Moreover, forehead injections involve distinct sensory innervation and skin thickness compared to other facial or cervical areas examined in prior studies, potentially explaining the observed gender-related variation.
Body mass index
At present, a significant relationship was found between BMI and pain. In line with our findings, Wu-Fienberg et al. (2018) reported that as BMI increases, the distance between the skin surface and the underlying muscle fascia increases, which may affect the depth of injection and potentially influence pain perception during the procedure (20). On the other hand, a study that compared the incidence and characteristics of neck pain in patients receiving BoNT-A injections using different needle lengths showed that BMI did not significantly correlate with the incidence or characteristics of neck pain, suggesting that BMI may not be a major factor influencing pain perception during BoNT-A injections (21). This inconsistency across studies may be attributed to anatomical differences in injection sites, since subcutaneous fat distribution in the forehead differs from that of the neck or trunk. In our sample, participants with higher BMI likely experienced greater needle pressure or tissue resistance, intensifying pain perception. Additionally, localized edema and variations in vascularity may further modulate nociceptive responses, contributing to these differences.
Handedness
Bivariate correlations revealed a non-significant relationship between left- and right-side pain scores, indicating a general consistency in pain reporting across both sides of the forehead. In a larger study, Fouché et al. (2017) investigated pain asymmetry in 302 patients receiving botulinum toxin or soft tissue filler injections and found consistently greater discomfort on the left side, particularly among right-handed individuals (4). In a sample of 351 healthy individuals subjected to unpleasant heat stimulation on both hands, Lugo et al. found that pain ratings on a Visual Analog Scale (VAS) were significantly higher on the left hand compared to the right, suggesting right hemisphere dominance in pain processing (22). In cosmetic injections, mechanical and psychological factors such as anticipation of pain or practitioner hand dominance may influence perceived asymmetry. The subtle lateralized trend observed in our data could thus reflect both neurophysiological and procedural elements unique to aesthetic injections.
Needle size
In the present study, no significant statistical relationship was found between injection pain and needle size. In contrast, Alam et al. (2015) evaluated the effect of needle gauge on pain during botulinum toxin injections and found that 30-gauge needles caused more pain than 32-gauge needles (23). Kämmerer et al. (2024), in a study comparing pain perception during BoNT-A injections using 30G, 33G, and 34G needles in the head and neck region, indicated that patients reported less discomfort with 33G and 34G needles compared to 30G needles, with 34G needles causing the least discomfort. In fact, smaller gauge needles (33G and 34G) are associated with reduced pain perception during BoNT-A injections (24). Maytharakcheep et al. (2024) also reported that micro-hypodermic needles resulted in reduced pain and bruising compared to standard needles, while maintaining similar therapeutic efficacy (25).
The lack of association in our results may be due to the relatively uniform needle sizes used in this study, where most injections were performed with 33G needles, limiting comparative variability. Furthermore, patient factors such as anxiety or injection speed could have outweighed the minor mechanical differences between gauges, leading to non-significant findings. Abreu Venancio et al. showed that the use of a finer-gauge needle (A thinner needle) is associated with reduced tissue trauma, pain, and bleeding at the injection site. This, in turn, can lead to a lower incidence and severity of short-term, procedure-related headaches following the injection (26).
History of injection
At present, it is noteworthy that the number of prior injection sessions showed a statistical trend toward reducing pain asymmetry. However, the borderline significance of this finding necessitates caution in its interpretation and underscores the need for verification in larger cohorts. In a study conducted by Shymaa et al. (2019), prior exposure to botulinum toxin injections was associated with lower perceived pain intensity, suggesting a possible adaptation or desensitization effect that could influence patient comfort in therapeutic settings such as carpal tunnel treatment (27). In a systematic review of patient outcomes across both aesthetic and therapeutic settings, Meretsky et al. (2024) highlighted improved quality of life and high satisfaction rates following BoNT-A treatment, findings that align with the positive functional outcomes observed in our cohort (28). Turner-Stokes et al. (2025) found no significant correlation between a patient's history of prior BoNT-A injections and the reduction in pain scores. However, patients requiring more frequent injections tended to have higher baseline pain scores and a smaller reduction in pain scores over time (15).
Other factors, such as the professional skill of the physician, may also affect pain. Borba et al. (2022) examined the adverse effects of botulinum toxin injections and determined that complications are minimal when administered by proficient practitioners (29). Although their investigation focused on safety outcomes rather than discomfort, Kaplan et al. (2017) emphasized the necessity of a precise anatomical understanding of facial musculature to achieve optimal cosmetic results (30). Although their research did not directly address pain, it supports the idea that anatomical variations influence patient experiences, underscoring the importance of skilled practitioners and individualized treatment approaches.
In our population, individuals with repeated exposure likely developed psychological tolerance and reduced anxiety, decreasing perceived pain. Furthermore, consistent administration by a single experienced physician may have standardized technique and minimized procedural variability, contributing to lower pain asymmetry among experienced participants. Indeed, in the present study, the borderline significance of this association should be interpreted with caution and requires validation in larger studies.
Conclusion
Female participants and those with higher BMI reported greater discomfort, while previous injection experience appeared to mitigate pain asymmetry. These findings highlight the need for individualized injection strategies based on patient characteristics and anatomical variations to enhance comfort and satisfaction. Further research is recommended to clarify the underlying neurophysiological mechanisms of pain lateralization in aesthetic procedures.
Limitations
The sample was predominantly young, right-handed females, which may limit the generalizability of the findings to other populations. Second, all injections were performed by a single experienced physician, so the influence of operator variability on pain perception could not be assessed. Third, pain was measured immediately after injection using a subjective scale (VAS), which may be affected by individual perception and reporting bias. Finally, the cross-sectional design prevents assessment of long-term changes in pain perception or adaptation over multiple injection sessions. The sample size, while adequate for the primary paired analysis, limited the power for subgroup analyses (e.g., by gender, substance use). Findings from these exploratory subgroup comparisons should be interpreted with caution and require validation in larger, adequately powered studies.
Acknowledgement
The authors would like to express their gratitude to the nursing staff and administrators of the surgical department of 5 Azar Hospital and the private clinic in Gorgan for their invaluable cooperation and assistance in patient recruitment and data collection. We also extend our sincere thanks to all the participants who took part in this study.
Funding sources
This study is not supported/funded.
Ethical statement
The study protocol was approved by the Ethics Committee of Golestan University of Medical Sciences (No. IR.GOUMS.REC.1403.096). The study was conducted in accordance with the ethical standards of the institutional and national research committee and with the 1964 Helsinki Declaration and its later amendments.
Conflicts of interest
The manuscript has been read and approved by all authors. The authors affirm that the requirements for authorship have been met and that the manuscript represents honest and original work.
Author contributions
Valiollah Alishahi: Conceptualization, methodology, formal analysis, investigation, data curation, writing original draft, and project administration; Ali Alishahi: Methodology, validation, investigation, resources, writing review, editing, and supervision.
Data availability statement
The datasets generated and analyzed during the current study are not publicly available due to participant privacy considerations but are available from the corresponding author upon reasonable request.
Editorial: Original article |
Subject:
General medicine
Received: 2025/04/12 | Accepted: 2025/06/25 | Published: 2025/09/21
Received: 2025/04/12 | Accepted: 2025/06/25 | Published: 2025/09/21
References
1. Rho N-K, Han K-H, Kim H-S. An update on the cosmetic use of botulinum toxin: the pattern of practice among Korean dermatologists. Toxins. 2022;14(5):329. [View at Publisher] [DOI] [PMID] [Google Scholar]
2. Sunil SM, Babu BG, Deepthi S, Veerabhadrappa AC, Vadavadagi SV, Punde P. Botulinum toxin for the treatment of hyperfunctional lines of the forehead. J Int Soc Prev Community Dent. 2015;5(4):276-82. [View at Publisher] [DOI] [PMID] [Google Scholar]
3. Zargaran D, Zoller F, Zargaran A, Rahman E, Woollard A, Weyrich T, et al. Complications of cosmetic botulinum toxin A injections to the upper face: a systematic review and meta-analysis. Aesthet Surg J. 2022;42(5):NP327-NP36. [View at Publisher] [DOI] [PMID] [Google Scholar]
4. Fouché JJ, Van Loghem JAJ, Thuis J, De Heer LM, van Oijen MG. Left/right pain asymmetry with injectable cosmetic treatments for the face. Aesthet Surg J. 2017;37(6):708-14. [View at Publisher] [DOI] [PMID] [Google Scholar]
5. Pud D, Golan Y, Pesta R. Hand dominancy-a feature affecting sensitivity to pain. Neurosci Lett. 2009;467(3):237-40. [View at Publisher] [DOI] [PMID] [Google Scholar]
6. Symonds LL, Gordon NS, Bixby JC, Mande MM. Right-lateralized pain processing in the human cortex: an FMRI study. J Neurophysiol. 2006;95(6):3823-30. [View at Publisher] [DOI] [PMID] [Google Scholar]
7. Wee SY, Park ES. Immunogenicity of botulinum toxin. Arch Plast Surg. 2022;49(1):12-8. [View at Publisher] [DOI] [PMID] [Google Scholar]
8. Nigam PK, Nigam A. Botulinum toxin. Indian journal of dermatology. 2010;55(1):8-14. [View at Publisher] [DOI] [PMID] [Google Scholar]
9. Sorensen EP, Urman C. Cosmetic complications: rare and serious events following botulinum toxin and soft tissue filler administration. J Drugs Dermatol. 2015;14(5):486-91. [View at Publisher] [PMID] [Google Scholar]
10. Ayoub N. Botulinum toxin therapy: a comprehensive review on clinical and pharmacological insights. J Clin Med. 2025;14(6):2021. [View at Publisher] [DOI] [PMID] [Google Scholar]
11. Fonfria E, Maignel J, Lezmi S, Martin V, Splevins A, Shubber S, et al. The expanding therapeutic utility of botulinum neurotoxins. Toxins. 2018;10(5):208. [View at Publisher] [DOI] [PMID] [Google Scholar]
12. Molaei A, Hemmati M, Izadi S, Paknazar F, Shakeri S, Hemmati H. Response to treatment with Botulinum toxin-A in patients with Refractory Chronic Migraine. Iran South Med J. 2024;27(1):1-12. [View at Publisher] [DOI] [Google Scholar]
13. Aoki KR. Evidence for antinociceptive activity of botulinum toxin type A in pain management. Headache. 2013;43(1):9-15. [View at Publisher] [DOI] [PMID] [Google Scholar]
14. Dima L, Bălan A, Moga MA, Dinu CG, Dimienescu OG, Varga I, et al. Botulinum toxin a valuable prophylactic agent for migraines and a possible future option for the prevention of hormonal variations-triggered migraines. Toxins. 2019;11(8):465. [View at Publisher] [DOI] [PMID] [Google Scholar]
15. Turner-Stokes L, Buchwald K, Ashford SA, Fheodoroff K, Jacinto J, Narayanan A, et al. Pain reduction with repeated injections of botulinum toxin A in upper limb spasticity: a longitudinal analysis from the ULIS-III study. Toxins. 2025;17(3):117. [View at Publisher] [DOI] [PMID] [Google Scholar]
16. Atraszkiewicz D. The processes underlying chronic migraine pathophysiology and its treatment with botulinum toxin type A. Neurol Clin Neurosci. 2021;9(6):421-9. [View at Publisher] [DOI] [Google Scholar]
17. Bravo BSF, de Melo Carvalho R, Gallo BF, Bravo LG. A retrospective study supporting the importance of individualizing the dose of botulinum toxin according to the age. J Cutan Aesthet Surg. 2021;14(1):88-92. [View at Publisher] [DOI] [PMID] [Google Scholar]
18. Santana L, Liu C. Experience of botulinum toxin A injections for chronic migraine headaches in a pediatric chronic pain clinic. J Pediatr Pharmacol Ther. 2021;26(2):151-6. [View at Publisher] [DOI] [PMID] [Google Scholar]
19. Kahn A, Bertin H, Corre P, Praud M, Paré A, Kün-Darbois J-D. Assessing the effectiveness of botulinum toxin injections into masticatory muscles in the treatment of temporomandibular disorders. J Oral Med Oral Sug. 2018;24(3):107-11. [View at Publisher] [DOI] [Google Scholar]
20. Wu-Fienberg Y, Ansari H, Zardouz S, Narouze S, Blaha T, Swanson M, et al. Anatomical look into onabotulinumtoxinA injection for chronic migraine headache. Reg Anesth Pain Med. 2018;43(8):869-74. [View at Publisher] [DOI] [PMID] [Google Scholar]
21. Dermitzakis EV, Vikelis M, Vlachos GS, Argyriou AA. Prospective comparison of longer needle lengths to assess the risk of onabotulinumtoxinA-associated neck pain in patients with chronic migraine. Toxins. 2022;14(7):434. [View at Publisher] [DOI] [PMID] [Google Scholar]
22. Lugo M, Istúriz G, Lara C, García N, Eblen-Zajjur A. Sensory lateralization in pain subjective perception for noxious heat stimulus. Somatosens Mot Res. 2002;19(3):207-12. [View at Publisher] [DOI] [PMID] [Google Scholar]
23. Alam M, Geisler A, Sadhwani D, Goyal A, Poon E, Nodzenski M, et al. Effect of needle size on pain perception in patients treated with botulinum toxin type A injections: a randomized clinical trial. JAMA Dermatol. 2015;151(11):1194-9. [View at Publisher] [DOI] [PMID] [Google Scholar]
24. Kämmerer TA, Bertlich R, Hartmann D, Jakob M, Weiss BG, Bertlich I, et al. Subjective discomfort during botulinumtoxin injections dependent on injection site and needle size: A comparison between 30g, 33g and 34g needles. Aesthetic Plast Surg. 2024;48(13):2528-35. [View at Publisher] [DOI] [PMID] [Google Scholar]
25. Maytharakcheep S, Phokaewvarangkul O, Bhidayasiri R. Does needle size matter? Effects of micro-hypodermic needle injections of botulinum toxin type A in patients with hemifacial spasm. Parkinsonism Relat Disord. 2024;118:105950. [View at Publisher] [DOI] [PMID] [Google Scholar]
26. de Abreu Venancio R, Guedes Pereira Alencar F, Zamperini C. Botulinum toxin, lidocaine, and dry-needling injections in patients with myofascial pain and headaches. Cranio. 2009;27(1):46-53. [View at Publisher] [DOI] [PMID] [Google Scholar]
27. Hablas SA, Nada DW, Alashkar DS, Elsharkawy AA. The effect of botulinum toxin type A injection in decreasing intratunnel tendon tension in carpal tunnel syndrome: a randomized controlled trial for efficacy and safety. Egypt. Rheumatol. Rehabil. 2019;46(4):299-303. [View at Publisher] [DOI] [Google Scholar]
28. Meretsky CR, Umali JP, Schiuma AT. A systematic review and comparative analysis of botox treatment in aesthetic and therapeutic applications: advantages, disadvantages, and patient outcomes. Cureus. 2024;16(8):e67961. [View at Publisher] [DOI] [PMID] [Google Scholar]
29. Borba A, Matayoshi S, Rodrigues M. Avoiding complications on the upper face treatment with botulinum toxin: a practical guide. Aesthetic plastic surgery. 2022;46(1):385-94. [View at Publisher] [DOI] [PMID] [Google Scholar]
30. Kaplan JB. Consideration of muscle depth for botulinum toxin injections: a three-dimensional approach. Plast Surg Nurs. 2017;37(1):32-8. [View at Publisher] [DOI] [PMID] [Google Scholar]
Send email to the article author
| Rights and permissions | |
 |
This work is licensed under a Creative Commons Attribution-NonCommercial 4.0 International License. |
