
Volume 12, Issue 4 (12-2024)
Jorjani Biomed J 2024, 12(4): 1-4 |
Back to browse issues page

Download citation:
BibTeX | RIS | EndNote | Medlars | ProCite | Reference Manager | RefWorks
Send citation to:



BibTeX | RIS | EndNote | Medlars | ProCite | Reference Manager | RefWorks
Send citation to:
Mirkarimi K, Shahini N, Rajabi A, Izadyar A H. The impact of self-care education on self-esteem, self-care behavior, and blood glucose levels in people with type 2 diabetes mellitus and pre-diabetes attending rural health centers in Gorgan City in 2023. Jorjani Biomed J 2024; 12 (4) :1-4
URL: http://goums.ac.ir/jorjanijournal/article-1-1001-en.html
URL: http://goums.ac.ir/jorjanijournal/article-1-1001-en.html



1- Nursing Research Center, Golestan University of Medical Sciences, Gorgan, Iran , ak.mirkarimi@gmail.com
2- Golestan Research Center of Psychiatry, Golestan University of Medical Sciences, Gorgan, Iran
3- Department of Biostatistics and Epidemiology, Faculty of Health, Golestan University of Medical Sciences, Gorgan, Iran
4- Nursing Research Center, Golestan University of Medical Sciences, Gorgan, Iran
2- Golestan Research Center of Psychiatry, Golestan University of Medical Sciences, Gorgan, Iran
3- Department of Biostatistics and Epidemiology, Faculty of Health, Golestan University of Medical Sciences, Gorgan, Iran
4- Nursing Research Center, Golestan University of Medical Sciences, Gorgan, Iran
Full-Text [PDF 435 kb]
(1602 Downloads)
| Abstract (HTML) (6381 Views)
Discussion
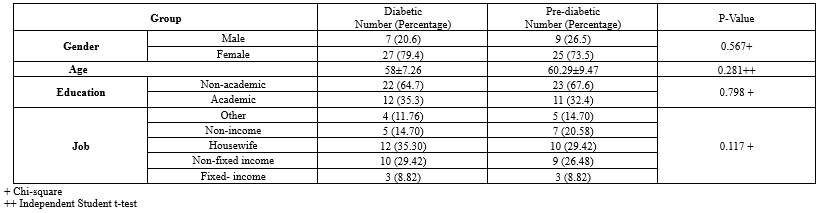
In this study, a total of 68 patients with T2DM, including 34 in the T2DM group and 34 in the pre-diabetes group, were enrolled. Similarly, in the study by Mahdi et al. (28), a total of 64 patients, including 32 T2DM and 32 pre-diabetes subjects, were included. The mean age of the participants in the current study was 59.15 ± 8.37, while in the study by Bagheri et al. (17)., this number was 66.85 ± 7.61. In the present study, no statistically significant differences were observed between the two groups in terms of age, gender, education, and occupation, which is consistent with other studies (16,21,22). This may indicate the absence of bias in the selection of study arms and the similar conditions of the samples at the start of the study.
Self-care
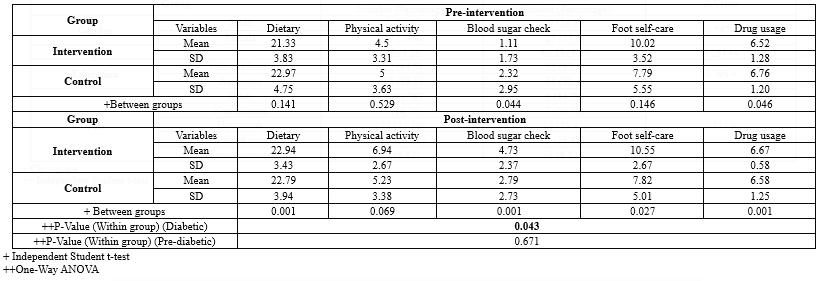
Prior to the intervention, there was a statistically significant difference in blood sugar levels and medication consumption between the two groups, which could be due to the presence of a control group in the pre-diabetes stage. This result was anticipated by researchers. However, what researchers were seeking was the difference in other self-care behaviors such as dietary regimen, physical activity, and foot care. Following the intervention, all self-care behaviors improved except for physical activity, which may be due to the fact that most of the samples studied were housewives with low levels of education and limited access to a suitable physical activity environment.
In a study conducted by Parham et al. (21), the findings also showed that 63% of patients with diabetes did not fully adhere to the prescribed dietary regimen, and 38% of them consumed suitable amounts of fruits and vegetables, while only 11% of them completely avoided high-fat foods such as red meat and high-fat dairy products. Moreover, 26% of patients with T2DM had no physical activity during the week, and only 2% of them participated in a specific exercise activity every day of the week. Interestingly, 35% of them did not check their blood sugar levels on any day of the week. Based on the results, 50% of them performed foot examinations seven days a week, which is in consistent with the present study regarding self-care behaviors. The findings of the study by Hamadzadeh and colleagues (22) showed that the highest level of adherence to self-care was in the dimensions of regular insulin or oral anti-diabetic medication use and adherence to the dietary regimen, and the patients exhibited the weakest self-care behavior in terms of regular blood glucose monitoring. In the present study, patients had a weak self-care score, which correlates with other studies (23) that indicate the need for different education than routine education provided in the healthcare system.
Self-esteem
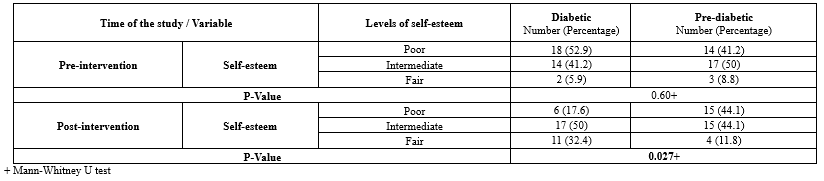
Before the intervention, 52.9% were weak, 41.2% were moderate, and 5.9% were strong in terms of self-esteem classification. After the intervention, 17.6% were weak, 50% were moderate, and 32.4% were strong. In Elalem et al.’s study, before the intervention, 85.3%, 14.7%, and 0% were weak, moderate, and strong, respectively, and after the intervention, these numbers reached 23.5%, 47.1%, and 29.4% (24), which the changes were statistically significant in both studies. In this regard, Solhi et al. reported a significant difference between the average self-esteem score before and after the intervention in the intervention group (23). This study demonstrated that the self-care program will cause a significant increase in self-esteem, which was in accordance with the results of studies by Elalem et al. (24) and Bagheri et al. (17). In the present study, it was shown that the self-esteem score significantly increased before and after the intervention in the intervention group, which was in accordance with the findings of the Elalem et al. (24). Also, Rahimi et al. (25) investigated the effect of the continuous care model on the self-esteem of heart failure patients and found a positive effect on self-esteem levels. Guillon et al. (26) investigated the relationship between self-esteem and mental disorders in adolescents. They found that mental disorders in adolescents are associated with low self-esteem, and appropriate therapeutic interventions can increase adolescent self-esteem. It was also reported in the study of Hashemi et al. (27) that the complications of diseases may lead to emotional and social discomfort, which may lead to a decrease in self-esteem, sadness, and social isolation.
Blood sugar
This study showed that the blood sugar level before and after the intervention was remarkably reduced in the intervention group, which was in accordance with the findings of Mahdi et al.’s study (28). In the investigation of Myers et al., it was proven that the quality of life of people with T2DM increased with training, which led to the control of blood sugar in these people. The dramatic decrease in the amount of sugar in the intervention group was an indicator of better blood sugar control of the elderly during the study period and positive changes in their behavior. These changes can be the most important factor in improving the quality of life (29). In the study of Ong-Artborira et al. (13), after performing linear regression and adjusting for gender, age, education, duration of diabetes, smoking, and alcohol consumption, it was shown that blood sugar levels were related to diabetes health literacy, self-efficacy, and self-care behavior. In the opposite results, Foppa et al. (14), in a study entitled “The effect of patient management on blood sugar control, adherence to self-care and knowledge about diabetes”, showed improvement in blood sugar control, adherence to self-care, and knowledge of T2DM in the study participants. Adhering to self-care can be challenging for many people with T2DM because it requires commitment and ongoing effort. In fact, as mentioned above, better implementation of self-care leads to greater commitment to the treatment of T2DM (14,30,31).
Conclusion
In the current study, the present intervention led to the improvement of self-esteem and self-care scores in people with T2DM and pre-diabetes. In fact, the lack of educational interventions in the country's health system, especially in the field of self-care and self-esteem, can represent the inappropriate conditions of patients with T2DM. Notably, the self-esteem scores of pre-diabetic patients were higher than those of T2DM patients, possibly because pre-diabetic individuals perceive themselves as less vulnerable to the challenges and potential complications associated withT2DM. Nevertheless, this issue can be considered a threat and more attention should be paid in future researches regarding providing education and sensitizing these people.
Acknowledgement
The author extends gratitude to all patients and those who provided required information of patients in the Health Houses.
Funding sources
The study protocol was financially supported by Golestan University of Medical Sciences.
Ethical statement
The study protocol was approved by the Ethical Committee of Golestan University of Medical Sciences (IR.GOUMS.REC.1402.029).
Conflicts of interest
The authors declare no competing interests.
Author contributions
Dr Mirkarimi and Amir Hosein Izadyar: Conceptualization and designing the
Manuscript/data gathering. Najmeh Shahini: Supervision and consulting in preparation of the protocol. Abdolhalim Rajabi: Methodology including Analyzing and interpreting the data.
Full-Text: (864 Views)
Introduction
Type 2 diabetes mellitus (T2DM) has imposed increasing burdens on healthcare systems worldwide (1). Prediabetes is characterized by fasting blood sugar equal to or greater than 100 and less than 126 mg/dL. Also, blood sugar above 126 mg/dL is considered diabetes (2). The prevalence of T2DM is rapidly increasing globally, at a rate of 3-4 percent per year (3). The Middle East is likely to face a significant increase in the burden of diabetes in the coming years. Additionally, the majority of the increase is expected to occur among individuals aged 45 to 64, who are economically considered part of the active population in their countries (4). The prevalence of diabetes in Iran has continuously expanded in recent years due to aging, obesity, urbanization, population growth, and sedentary lifestyles. Studies have shown that 11.4% of the Iranian population has been diagnosed with diabetes (5), with nearly 40% of them still undiagnosed (4). Currently, T2DM is one of the main causes of mortality and reduced life expectancy (6). Chronic hyperglycemia resulting from it leads to macro- and microvascular complications. Despite numerous complications such as heart disease, diabetic retinopathy, stroke, and amputation, proper control and care can prevent these serious disabilities (3).
Self-esteem is a part of an individual's self-concept, which includes cognitive, behavioral, and emotional aspects. More precisely, self-esteem refers to the level of value that individuals place on themselves. The behavioral aspects of self-esteem manifest in behaviors such as assertiveness, decisiveness, and politeness toward others (7). Self-esteem has a very close relationship with an individual's mental image of themselves and their coping mechanisms. In other words, a positive self-image leads to a sense of worthiness in the individual. Illness, treatments, or related side effects can lead to changes in mental self-image and self-esteem, which are much more apparent in chronic diseases due to their long and unpredictable nature (8). Additionally, coping mechanisms that play a crucial role in enabling a patient to learn to live with the disease are also influenced by self-esteem (9). Chronic diseases such as diabetes and hypertension present individuals with various challenges, including pain, physical activity disorders, lifestyle changes, and reduced self-esteem. Self-esteem is an important factor in coping with stressful factors in chronic diseases, as higher self-esteem leads to better adaptation to the disease regardless of its type and severity (10). Low self-esteem in chronic diseases negatively affects interpersonal relationships, thinking, feelings, and patient performance. Numerous studies on individuals with chronic diseases such as diabetes, cardiovascular diseases, arthritis, malignancies, and respiratory diseases have shown an increase in depressive symptoms. High self-esteem is associated with lower levels of depression in chronic diseases, making its assessment important in chronic diseases such as diabetes and hypertension (11). A survey conducted by Helgeson et al. on patients with diabetes reported that low self-esteem had negative effects on the self-care of the patients (12). Several studies have suggested that self-care behaviors are a determinant of disease control and related health complications (13). A study carried out on navigation of patients with T2DM indicated that the group accompanied for guidance and education as a stimulus to adherence to treatment obtained positive results with reduced HbA1c levels, better adherence to treatments, and lower body mass index after 12 weeks of intervention (14)
Many patients have emphasized the importance of blood sugar control as a key factor to control and treat T2DM due to increased knowledge in the field of diabetes. The main goal of diabetes treatment is to reduce and maintain serum glucose in the normal range (15). Self-care is defined as a strategy to adapt to events and stresses of life, which improves health and includes special activities that alleviate the symptoms of the disease (16). Therefore, this study aimed to determine the impact of self-care education on self-esteem, self-care behavior, and blood glucose levels in patients with T2DM and those in the pre-diabetic stage attending rural health centers in Gorgan City in 2023.
Methods
Study procedure
A quasi-experimental, pre-and post-test intervention study was conducted on 68 patients with T2DM and patients in the pre-diabetic stage visiting healthcare centers covered by rural health centers in Gorgan City. At present, a multistage sampling technique was used to collect data. Two Health Houses were included in the study, randomly. Then, 68 patients were also randomly selected in each group (34 patients in T2DM group and 34 participants in the pre-diabetes group) from two separate Health Houses. The study protocol was approved by the Ethics Committee of Golestan University of Medical Sciences (Ethics no: IR.GOUMS.REC.1402.029). Before the study, all participants filled out an informed consent form and were informed that they could withdraw from the study at any time if they wished.
Participants
Individuals with a minimum of one year of illness, reading and writing abilities, and age 30 and above were included in the study. Additionally, absence from two or more educational sessions and individuals' lack of interest in continuing participation were considered exclusion criteria of the study. The groups were selected from two separate rural health centers to prevent contact between patients and the prevention of forming probable bias.
Intervention of the study
Each group (T2DM, and pre-diabetes) was divided into three subgroups to conduct the training in two study groups. Each group consisted of ten people except for one group which had to be 12 people due to circumstances (Total of 34 patients). Health education specialists applied diabetes education based on the guidelines of the Brazilian Diabetes Society that considered the following subjects: subcutaneous drug administration, prescribed drugs, foot care and improvement in coping, activities/exercise prescribed, improvement in willingness to learn, diet planning, and assistance to stop smoking when present support for decision-making, guidelines regarding eye fundus examination, vaccination, and review on medication adherence, adherence to self-monitoring, and agreed goals (14). The training sessions were conducted in 30- to 45-minute sessions, and educational pamphlets were distributed among the patients, and, in brief, at the end of the sessions, individuals' questions were answered if needed. All educations were provided by a health education specialist.
Sample size
Based on the study by Bagheri et al. (17) association between self-care behaviors and self-esteem of rural elderlies’ necessity of health promotion with a 95% confidence level and a minimum test power of 80%, a minimum of 62 samples were required. Taking into account a 10% dropout rate during the follow-up process, a minimum of 68 samples (34 in each group) were included in the study. In total, 34 diabetic patients (Blood sugar level >126 mg/dl) and 34 pre-diabetic patients (Blood sugar level 100 to 125 mg/dl) (18) were studied. Diabetic and pre-diabetic patients with health records in the health center were included in the study using simple random sampling.
Instrument of the study
To collect data, a demographic information questionnaire (Age, gender, marital status, education level, and occupation), the Summary of Diabetes Self-care Activities (SDSCA) questionnaire (19) with a reliability of 0.95, and the Coopersmith Self-esteem Inventory (20) with a reliability of 0.88 were used. The self-care questionnaire included 12 questions (Five items about diet, two about exercise, two about blood sugar control, two about foot care, and one about diabetic medication adherence and FBS levels) based on the patient's most recent test within the past week. For each of the questions, a score of 1 was given for performing the self-care behavior daily, and a score of 0 was given for not performing it (The score ranges from a maximum of 7 and a minimum of 0 for each question over a week). The standard Coopersmith Self-esteem Inventory consists of 58 items, and the respondent must mark each item with "Yes" or "No" to indicate whether it applies to them. The items are categorized into the general scale (26 items), social scale (8 items), family scale (8 items), educational or occupational scale (8 items), and lie scale (8 items).
Statistical analyses
The data were described using mean and standard deviation, the assumptions of all statistical tests, including homogeneity of variances (assessed via Levene’s test) and normality (assessed via the Kolmogorov-Smirnov test), were checked and met. The data were then analyzed using the Chi-square test for categorical variables, Independent Student Samples T-test for between-group comparisons, and analyzed by Kolmogorov-Smirnov, Chi-square, Independent T-test, and Paired T-test. The significance level for the tests was considered to be less than 0.05.
Results
The mean age in the T2DM group was 58 ±7.26, and 60.29 ± 9.47 years in the pre-diabetes group. In the T2DM group, 23 individuals (67.6%) and in the pre-diabetes group, 22 individuals (64.7%) had education beyond high school diploma. Also, the majority of patients in the T2DM group 12 (35.30) were housewives compared to 10 (29.42) in the pre-diabetic group (Table 1). In this study, before the intervention, a significant difference was observed between the two groups only in terms of self-care behaviors for blood glucose monitoring (P-Value =0.044) and medication adherence (P-Value =0.046). However, after the intervention, significant differences were observed in blood glucose monitoring (P-Value =0.001), foot care (P-Value =0.027), and medication adherence (P-Value =0.001) (Table 2).
In the T2DM group, post-intervention self-esteem classification revealed that moderate self-esteem was the most frequent with a frequency of 17 individuals (50%), and it had a trend of moderate and low self-esteem with a frequency of 15 individuals (44.1%) in the pre-diabetes group, with a statistically significant difference between the two groups (P-Value =0.027) (Table 3). The blood glucose level did not indicate a statistically significant difference in the pre-diabetes group before and after the intervention (P-Value=0.256), while the blood glucose level was statistically significant in the T2DM group before and after the intervention (P-Value=0.001) (Table 4).
Type 2 diabetes mellitus (T2DM) has imposed increasing burdens on healthcare systems worldwide (1). Prediabetes is characterized by fasting blood sugar equal to or greater than 100 and less than 126 mg/dL. Also, blood sugar above 126 mg/dL is considered diabetes (2). The prevalence of T2DM is rapidly increasing globally, at a rate of 3-4 percent per year (3). The Middle East is likely to face a significant increase in the burden of diabetes in the coming years. Additionally, the majority of the increase is expected to occur among individuals aged 45 to 64, who are economically considered part of the active population in their countries (4). The prevalence of diabetes in Iran has continuously expanded in recent years due to aging, obesity, urbanization, population growth, and sedentary lifestyles. Studies have shown that 11.4% of the Iranian population has been diagnosed with diabetes (5), with nearly 40% of them still undiagnosed (4). Currently, T2DM is one of the main causes of mortality and reduced life expectancy (6). Chronic hyperglycemia resulting from it leads to macro- and microvascular complications. Despite numerous complications such as heart disease, diabetic retinopathy, stroke, and amputation, proper control and care can prevent these serious disabilities (3).
Self-esteem is a part of an individual's self-concept, which includes cognitive, behavioral, and emotional aspects. More precisely, self-esteem refers to the level of value that individuals place on themselves. The behavioral aspects of self-esteem manifest in behaviors such as assertiveness, decisiveness, and politeness toward others (7). Self-esteem has a very close relationship with an individual's mental image of themselves and their coping mechanisms. In other words, a positive self-image leads to a sense of worthiness in the individual. Illness, treatments, or related side effects can lead to changes in mental self-image and self-esteem, which are much more apparent in chronic diseases due to their long and unpredictable nature (8). Additionally, coping mechanisms that play a crucial role in enabling a patient to learn to live with the disease are also influenced by self-esteem (9). Chronic diseases such as diabetes and hypertension present individuals with various challenges, including pain, physical activity disorders, lifestyle changes, and reduced self-esteem. Self-esteem is an important factor in coping with stressful factors in chronic diseases, as higher self-esteem leads to better adaptation to the disease regardless of its type and severity (10). Low self-esteem in chronic diseases negatively affects interpersonal relationships, thinking, feelings, and patient performance. Numerous studies on individuals with chronic diseases such as diabetes, cardiovascular diseases, arthritis, malignancies, and respiratory diseases have shown an increase in depressive symptoms. High self-esteem is associated with lower levels of depression in chronic diseases, making its assessment important in chronic diseases such as diabetes and hypertension (11). A survey conducted by Helgeson et al. on patients with diabetes reported that low self-esteem had negative effects on the self-care of the patients (12). Several studies have suggested that self-care behaviors are a determinant of disease control and related health complications (13). A study carried out on navigation of patients with T2DM indicated that the group accompanied for guidance and education as a stimulus to adherence to treatment obtained positive results with reduced HbA1c levels, better adherence to treatments, and lower body mass index after 12 weeks of intervention (14)
Many patients have emphasized the importance of blood sugar control as a key factor to control and treat T2DM due to increased knowledge in the field of diabetes. The main goal of diabetes treatment is to reduce and maintain serum glucose in the normal range (15). Self-care is defined as a strategy to adapt to events and stresses of life, which improves health and includes special activities that alleviate the symptoms of the disease (16). Therefore, this study aimed to determine the impact of self-care education on self-esteem, self-care behavior, and blood glucose levels in patients with T2DM and those in the pre-diabetic stage attending rural health centers in Gorgan City in 2023.
Methods
Study procedure
A quasi-experimental, pre-and post-test intervention study was conducted on 68 patients with T2DM and patients in the pre-diabetic stage visiting healthcare centers covered by rural health centers in Gorgan City. At present, a multistage sampling technique was used to collect data. Two Health Houses were included in the study, randomly. Then, 68 patients were also randomly selected in each group (34 patients in T2DM group and 34 participants in the pre-diabetes group) from two separate Health Houses. The study protocol was approved by the Ethics Committee of Golestan University of Medical Sciences (Ethics no: IR.GOUMS.REC.1402.029). Before the study, all participants filled out an informed consent form and were informed that they could withdraw from the study at any time if they wished.
Participants
Individuals with a minimum of one year of illness, reading and writing abilities, and age 30 and above were included in the study. Additionally, absence from two or more educational sessions and individuals' lack of interest in continuing participation were considered exclusion criteria of the study. The groups were selected from two separate rural health centers to prevent contact between patients and the prevention of forming probable bias.
Intervention of the study
Each group (T2DM, and pre-diabetes) was divided into three subgroups to conduct the training in two study groups. Each group consisted of ten people except for one group which had to be 12 people due to circumstances (Total of 34 patients). Health education specialists applied diabetes education based on the guidelines of the Brazilian Diabetes Society that considered the following subjects: subcutaneous drug administration, prescribed drugs, foot care and improvement in coping, activities/exercise prescribed, improvement in willingness to learn, diet planning, and assistance to stop smoking when present support for decision-making, guidelines regarding eye fundus examination, vaccination, and review on medication adherence, adherence to self-monitoring, and agreed goals (14). The training sessions were conducted in 30- to 45-minute sessions, and educational pamphlets were distributed among the patients, and, in brief, at the end of the sessions, individuals' questions were answered if needed. All educations were provided by a health education specialist.
Sample size
Based on the study by Bagheri et al. (17) association between self-care behaviors and self-esteem of rural elderlies’ necessity of health promotion with a 95% confidence level and a minimum test power of 80%, a minimum of 62 samples were required. Taking into account a 10% dropout rate during the follow-up process, a minimum of 68 samples (34 in each group) were included in the study. In total, 34 diabetic patients (Blood sugar level >126 mg/dl) and 34 pre-diabetic patients (Blood sugar level 100 to 125 mg/dl) (18) were studied. Diabetic and pre-diabetic patients with health records in the health center were included in the study using simple random sampling.
Instrument of the study
To collect data, a demographic information questionnaire (Age, gender, marital status, education level, and occupation), the Summary of Diabetes Self-care Activities (SDSCA) questionnaire (19) with a reliability of 0.95, and the Coopersmith Self-esteem Inventory (20) with a reliability of 0.88 were used. The self-care questionnaire included 12 questions (Five items about diet, two about exercise, two about blood sugar control, two about foot care, and one about diabetic medication adherence and FBS levels) based on the patient's most recent test within the past week. For each of the questions, a score of 1 was given for performing the self-care behavior daily, and a score of 0 was given for not performing it (The score ranges from a maximum of 7 and a minimum of 0 for each question over a week). The standard Coopersmith Self-esteem Inventory consists of 58 items, and the respondent must mark each item with "Yes" or "No" to indicate whether it applies to them. The items are categorized into the general scale (26 items), social scale (8 items), family scale (8 items), educational or occupational scale (8 items), and lie scale (8 items).
Statistical analyses
The data were described using mean and standard deviation, the assumptions of all statistical tests, including homogeneity of variances (assessed via Levene’s test) and normality (assessed via the Kolmogorov-Smirnov test), were checked and met. The data were then analyzed using the Chi-square test for categorical variables, Independent Student Samples T-test for between-group comparisons, and analyzed by Kolmogorov-Smirnov, Chi-square, Independent T-test, and Paired T-test. The significance level for the tests was considered to be less than 0.05.
Results
The mean age in the T2DM group was 58 ±7.26, and 60.29 ± 9.47 years in the pre-diabetes group. In the T2DM group, 23 individuals (67.6%) and in the pre-diabetes group, 22 individuals (64.7%) had education beyond high school diploma. Also, the majority of patients in the T2DM group 12 (35.30) were housewives compared to 10 (29.42) in the pre-diabetic group (Table 1). In this study, before the intervention, a significant difference was observed between the two groups only in terms of self-care behaviors for blood glucose monitoring (P-Value =0.044) and medication adherence (P-Value =0.046). However, after the intervention, significant differences were observed in blood glucose monitoring (P-Value =0.001), foot care (P-Value =0.027), and medication adherence (P-Value =0.001) (Table 2).
In the T2DM group, post-intervention self-esteem classification revealed that moderate self-esteem was the most frequent with a frequency of 17 individuals (50%), and it had a trend of moderate and low self-esteem with a frequency of 15 individuals (44.1%) in the pre-diabetes group, with a statistically significant difference between the two groups (P-Value =0.027) (Table 3). The blood glucose level did not indicate a statistically significant difference in the pre-diabetes group before and after the intervention (P-Value=0.256), while the blood glucose level was statistically significant in the T2DM group before and after the intervention (P-Value=0.001) (Table 4).

Discussion
In this study, a total of 68 patients with T2DM, including 34 in the T2DM group and 34 in the pre-diabetes group, were enrolled. Similarly, in the study by Mahdi et al. (28), a total of 64 patients, including 32 T2DM and 32 pre-diabetes subjects, were included. The mean age of the participants in the current study was 59.15 ± 8.37, while in the study by Bagheri et al. (17)., this number was 66.85 ± 7.61. In the present study, no statistically significant differences were observed between the two groups in terms of age, gender, education, and occupation, which is consistent with other studies (16,21,22). This may indicate the absence of bias in the selection of study arms and the similar conditions of the samples at the start of the study.
Self-care
Prior to the intervention, there was a statistically significant difference in blood sugar levels and medication consumption between the two groups, which could be due to the presence of a control group in the pre-diabetes stage. This result was anticipated by researchers. However, what researchers were seeking was the difference in other self-care behaviors such as dietary regimen, physical activity, and foot care. Following the intervention, all self-care behaviors improved except for physical activity, which may be due to the fact that most of the samples studied were housewives with low levels of education and limited access to a suitable physical activity environment.
In a study conducted by Parham et al. (21), the findings also showed that 63% of patients with diabetes did not fully adhere to the prescribed dietary regimen, and 38% of them consumed suitable amounts of fruits and vegetables, while only 11% of them completely avoided high-fat foods such as red meat and high-fat dairy products. Moreover, 26% of patients with T2DM had no physical activity during the week, and only 2% of them participated in a specific exercise activity every day of the week. Interestingly, 35% of them did not check their blood sugar levels on any day of the week. Based on the results, 50% of them performed foot examinations seven days a week, which is in consistent with the present study regarding self-care behaviors. The findings of the study by Hamadzadeh and colleagues (22) showed that the highest level of adherence to self-care was in the dimensions of regular insulin or oral anti-diabetic medication use and adherence to the dietary regimen, and the patients exhibited the weakest self-care behavior in terms of regular blood glucose monitoring. In the present study, patients had a weak self-care score, which correlates with other studies (23) that indicate the need for different education than routine education provided in the healthcare system.
Self-esteem
Before the intervention, 52.9% were weak, 41.2% were moderate, and 5.9% were strong in terms of self-esteem classification. After the intervention, 17.6% were weak, 50% were moderate, and 32.4% were strong. In Elalem et al.’s study, before the intervention, 85.3%, 14.7%, and 0% were weak, moderate, and strong, respectively, and after the intervention, these numbers reached 23.5%, 47.1%, and 29.4% (24), which the changes were statistically significant in both studies. In this regard, Solhi et al. reported a significant difference between the average self-esteem score before and after the intervention in the intervention group (23). This study demonstrated that the self-care program will cause a significant increase in self-esteem, which was in accordance with the results of studies by Elalem et al. (24) and Bagheri et al. (17). In the present study, it was shown that the self-esteem score significantly increased before and after the intervention in the intervention group, which was in accordance with the findings of the Elalem et al. (24). Also, Rahimi et al. (25) investigated the effect of the continuous care model on the self-esteem of heart failure patients and found a positive effect on self-esteem levels. Guillon et al. (26) investigated the relationship between self-esteem and mental disorders in adolescents. They found that mental disorders in adolescents are associated with low self-esteem, and appropriate therapeutic interventions can increase adolescent self-esteem. It was also reported in the study of Hashemi et al. (27) that the complications of diseases may lead to emotional and social discomfort, which may lead to a decrease in self-esteem, sadness, and social isolation.
Blood sugar
This study showed that the blood sugar level before and after the intervention was remarkably reduced in the intervention group, which was in accordance with the findings of Mahdi et al.’s study (28). In the investigation of Myers et al., it was proven that the quality of life of people with T2DM increased with training, which led to the control of blood sugar in these people. The dramatic decrease in the amount of sugar in the intervention group was an indicator of better blood sugar control of the elderly during the study period and positive changes in their behavior. These changes can be the most important factor in improving the quality of life (29). In the study of Ong-Artborira et al. (13), after performing linear regression and adjusting for gender, age, education, duration of diabetes, smoking, and alcohol consumption, it was shown that blood sugar levels were related to diabetes health literacy, self-efficacy, and self-care behavior. In the opposite results, Foppa et al. (14), in a study entitled “The effect of patient management on blood sugar control, adherence to self-care and knowledge about diabetes”, showed improvement in blood sugar control, adherence to self-care, and knowledge of T2DM in the study participants. Adhering to self-care can be challenging for many people with T2DM because it requires commitment and ongoing effort. In fact, as mentioned above, better implementation of self-care leads to greater commitment to the treatment of T2DM (14,30,31).
Conclusion
In the current study, the present intervention led to the improvement of self-esteem and self-care scores in people with T2DM and pre-diabetes. In fact, the lack of educational interventions in the country's health system, especially in the field of self-care and self-esteem, can represent the inappropriate conditions of patients with T2DM. Notably, the self-esteem scores of pre-diabetic patients were higher than those of T2DM patients, possibly because pre-diabetic individuals perceive themselves as less vulnerable to the challenges and potential complications associated withT2DM. Nevertheless, this issue can be considered a threat and more attention should be paid in future researches regarding providing education and sensitizing these people.
Acknowledgement
The author extends gratitude to all patients and those who provided required information of patients in the Health Houses.
Funding sources
The study protocol was financially supported by Golestan University of Medical Sciences.
Ethical statement
The study protocol was approved by the Ethical Committee of Golestan University of Medical Sciences (IR.GOUMS.REC.1402.029).
Conflicts of interest
The authors declare no competing interests.
Author contributions
Dr Mirkarimi and Amir Hosein Izadyar: Conceptualization and designing the
Manuscript/data gathering. Najmeh Shahini: Supervision and consulting in preparation of the protocol. Abdolhalim Rajabi: Methodology including Analyzing and interpreting the data.
Type of Article: Original article |
Subject:
Health
Received: 2023/11/27 | Accepted: 2024/06/10 | Published: 2025/09/2
Received: 2023/11/27 | Accepted: 2024/06/10 | Published: 2025/09/2
References
1. Yahaya TO, Oladele EO, Mshelia MB, Sifau MO, Fashola OD, Bunza M, et al. Influence of ABO blood groups and demographic characteristics on the prevalence of type 2 diabetes in Lagos, southwest Nigeria. Bulletin of the National Research Centre. 2021;45(1):144. [View at Publisher] [DOI] [Google Scholar]
2. Okada A, Kaneko H, Matsuoka S, Itoh H, Suzuki Y, Fujiu K, et al. Association of cardiovascular health metrics with annual incidence of prediabetes or diabetes: Analysis of a nationwide real‐world database. J Diabetes Investig. 2023;14(3):452-62. [View at Publisher] [DOI] [PMID] [Google Scholar]
3. Haris B, Saraswathi S, Al‐Khawaga S, Hasnah R, Saeed A, Mundekkadan S, et al. Epidemiology, genetic landscape and classification of childhood diabetes mellitus in the State of Qatar. J Diabetes Investig. 2021;12(12):2141-8. [View at Publisher] [DOI] [PMID] [Google Scholar]
4. Davari M, Bayazidi Y, Kebriaeezadeh A, Esteghamati A, Bandarian F, Kashi Z, et al. Quality of care in type 2 diabetes in Iran; a cross-sectional study using patient-level data. BMC Endocr Disord. 2022;22(1):133. [View at Publisher] [DOI] [PMID] [Google Scholar]
5. Esteghamati A, Etemad K, Koohpayehzadeh J, Abbasi M, Meysamie A, Noshad S, et al. Trends in the prevalence of diabetes and impaired fasting glucose in association with obesity in Iran: 2005-2011. Diabetes Res Clin Pract. 2014;103(2):319-27. [View at Publisher] [DOI] [PMID] [Google Scholar]
6. Shahabi N, Kolivand M, Salari N, Abbasi P. The effect of telenursing training based on family-centered empowerment pattern on compliance with diet regimen in patients with diabetes mellitus type 2: a randomized clinical trial. BMC Endocr Disord. 2022;22(1):36. [View at Publisher] [DOI] [PMID] [Google Scholar]
7. Farahati M, Fathi-Ashtiani A, Moradi A. Relationship between family communication patterns and locus of control and self-esteem in adolescents. Journal of Behavioral Sciences. 2011;5(3):279-85. [View at Publisher] [Google Scholar]
8. Mirzaei Alavijeh M, Rajaei N, Rezaei F, Hasanpoor S, Pirouzeh R, Babaei Borzabadi M. Comparison of self-esteem, locus of control and their relationship with university students' educational status at Shahid Sadoughi University of Medical Sciences-Yazd. Journal of Medical Education and Development. 2012;7(1):58-70. [View at Publisher] [Google Scholar]
9. Lee TH, Kim TH, Kim W, Park E. Effects of difference in self-esteem between spouses on depressive symptom: Result from a data nationally representative of South Korean. Psychiatry Res. 2016;246:623-8. [View at Publisher] [DOI] [PMID] [Google Scholar]
10. Bisschop MI, Kriegsman DM, Beekman AT, Deeg DJ. Chronic diseases and depression: the modifying role of psychosocial resources. Soc Sci Med. 2004;59(4):721-33. [View at Publisher] [DOI] [PMID] [Google Scholar]
11. Lukman NA, Leibing A, Merry L. Self-care experiences of adults with chronic disease in Indonesia: An integrative review. Int J Chronic Dis. 2020;2020:1379547. [View at Publisher] [DOI] [PMID] [Google Scholar]
12. Helgeson VS, Honcharuk E, Becker D, Escobar O, Siminerio L. A focus on blood glucose monitoring: relation to glycemic control and determinants of frequency. Pediatr Diabetes. 2011;12(1):25-30. [View at Publisher] [DOI] [PMID] [Google Scholar]
13. Ong-Artborirak P, Seangpraw K, Boonyathee S, Auttama N, Winaiprasert PJBg. Health literacy, self-efficacy, self-care behaviors, and glycemic control among older adults with type 2 diabetes mellitus: a cross-sectional study in Thai communities. BMC Geriatr. 2023;23(1):297. [View at Publisher] [DOI] [PMID] [Google Scholar]
14. Foppa L, Nemetz B, de Matos R, Schneiders J, Telo GH, Schaan BD. The impact of patient navigation on glycemic control, adherence to self-care and knowledge about diabetes: an intervention study. Diabetol Metab Syndr. 2023;15(1):172. [View at Publisher] [DOI] [PMID] [Google Scholar]
15. Maleka A, Khosravi S, Charkazi A, Pahlavanzaded B, Khosravi Z, Khosravi M. Relationship Relationship between self-care behaviors and glycosylated hemoglobin level in diabetic patients. Journal of Gorgan University of Medical Sciences. 2021;22(4):84-91. [View at Publisher] [Google Scholar]
16. Kheradmand A, Ranjbarzade A, H Hassanpour K, Bidi F. Effectiveness of educational program on knowledge, attitude, self care and life style in patients with type II diabetes. Journal of Sabzevar University of Medical Sciences. 2013;19(4):336-44. [View at Publisher] [Google Scholar]
17. Bagheri-Nesami M, Goudarzian AH, Mirani H, Jouybari SS, Nasiri D. Association between self-care behaviors and self-esteem of rural elderlies; necessity of health promotion. Mater Sociomed. 2016;28(1):41-5. [View at Publisher] [DOI] [PMID] [Google Scholar]
18. Azizi F, Hadaegh F. Population-based incidence of Type 2 diabetes and its associated risk factors: results from a six-year cohort study in Iran. Iranian Journal of Endocrinology and Metabolism. 2015;17(1):1-3. [View at Publisher] [DOI] [PMID] [Google Scholar]
19. Solhi M, Hazrati S, Nejaddadgar N. Analysis of Self-care Behaviors and their Related Factors in Patients with Type II Diabetes. J Diabetes Nurs. 2017;5(3):223-31. [View at Publisher] [DOI] [Google Scholar]
20. Soheylizad M, Yahaghi Amjad E, Amini D, Gholamaliee B. Relationship between self-esteem, resilience and quality of life in patients with type 2 diabetes in Hamadan in 2015. Pajouhan Sci J. 2016;15(1):1-8. [View at Publisher] [DOI] [Google Scholar]
21. Parham M, Riahin A, Jandaghi M, Darivandpour A. Self Care Behaviors of Diabetic Patients in Qom. 2013. Qom Univ Med Sci J. 2012;6(4):81-7. [View at Publisher] [Google Scholar]
22. Hamadzadeh S, Ezate G. A determination of self-care performance among diabetic patients in endocrine clinic of Taleghane hospital in Tehran. Iranian Journal of Nursing Research. 2014;8(4):11-8. [View at Publisher] [Google Scholar]
23. Solhi M, Hazrati S, Nejaddadgar N. Analysis of self-care behaviors and their related factors in patients with type II diabetes. J Diabetes Nurs. 2017;5(3):223-31. [View at Publisher] [DOI] [Google Scholar]
24. Abd Elalem SM, Shehata O, Shattla SI. The effect of self-care nursing intervention model on self-esteem and quality of life among burn patients. Clinical Nursing Studies. 2018;6(2):79-90. [View at Publisher] [DOI] [Google Scholar]
25. Rahimi A, Ahmadi F, Ghaliaf M. Effect of applying continuous care model on self-esteem in hemodialysis patients. J Adv Med Biomed Res. 2005:13(53):16-21. [View at Publisher] [Google Scholar]
26. Guillon M, Crocq MA, Bailey PE. The relationship between self-esteem and psychiatric disorders in adolescents. Eur Psychiatry. 2003;18(2):59-62. [View at Publisher] [DOI] [PMID] [Google Scholar]
27. Hashemi F, Dolatabad FR, Yektatalab S, Ayaz M, Zare N, Mansouri P. Effect of Orem Self-Care program on the life quality of burn patients referred to Ghotb-al-Din-e-Shirazi burn center, Shiraz, Iran: a randomized controlled trial. Int J Community Based Nurs Midwifery. 2014;2(1):40-50. [View at Publisher] [PMID] [Google Scholar]
28. Mahdi H, Maddah SMB, Mahammadi F. The effectiveness of self-care training on quality of life among elderlies with diabetes. Iranian Nursing Scientific Association. 2016;2(4):32-9. [View at Publisher] [DOI] [Google Scholar]
29. Myers VH, McVay MA, Brashear MM, Johannsen NM, Swift DL, Kramer K, et al. Exercise training and quality of life in individuals with type 2 diabetes: a randomized controlled trial. Diabetes care. 2013;36(7):1884-90. [View at Publisher] [DOI] [PMID] [Google Scholar]
30. Kim SH. Health literacy and diabetes self‐care activities: The mediating effect of knowledge and patient activation. Int J Nurs Pract. 2021;27(4):e12925. [View at Publisher] [DOI] [PMID] [Google Scholar]
31. Niguse H, Belay G, Fisseha G, Desale T, Gebremedhn GJ. Self-care related knowledge, attitude, practice and associated factors among patients with diabetes in Ayder Comprehensive Specialized Hospital, North Ethiopia. BMC Res Notes. 2019;12(1):34. [View at Publisher] [DOI] [PMID] [Google Scholar]
Send email to the article author
| Rights and permissions | |
 |
This work is licensed under a Creative Commons Attribution-NonCommercial 4.0 International License. |
