
Volume 8, Issue 2 (7-2020)
Jorjani Biomed J 2020, 8(2): 4-10 |
Back to browse issues page


Download citation:
BibTeX | RIS | EndNote | Medlars | ProCite | Reference Manager | RefWorks
Send citation to:



BibTeX | RIS | EndNote | Medlars | ProCite | Reference Manager | RefWorks
Send citation to:
Esmaeili M, Khosravi N, Habibi Kia A. Non-syndromic multiple supernumerary teeth: A case report. Jorjani Biomed J 2020; 8 (2) :4-10
URL: http://goums.ac.ir/jorjanijournal/article-1-721-en.html
URL: http://goums.ac.ir/jorjanijournal/article-1-721-en.html



1- Department of Oral and Maxillofacial Radiology, Faculty of Dentistry, Shahid Sadoughi University of Medical Sciences, Yazd, Iran
2- Deparment of Oral and Maxillofacial Radiology, Dental School, Lorestan University of Medical Sciences, Khorramabad, Iran
3- Department of Oral and MaxillofacialRadiology, Faculty of dentistry, Ahvaz Jundishapur University of Medical Sciences, Ahvaz, Iran , alihabibikia@yahoo.com
2- Deparment of Oral and Maxillofacial Radiology, Dental School, Lorestan University of Medical Sciences, Khorramabad, Iran
3- Department of Oral and MaxillofacialRadiology, Faculty of dentistry, Ahvaz Jundishapur University of Medical Sciences, Ahvaz, Iran , alihabibikia@yahoo.com
Keywords: Non-syndromic , Multiple supernumerary teeth , CBCT (cone beam computed tomography) , unerupted teeth [MeSH]
Full-Text [PDF 536 kb]
(1732 Downloads)
| Abstract (HTML) (3930 Views)

Fig1. The panoramic radiograph showed the presence of ten supernumerary teeth in all four quadrants
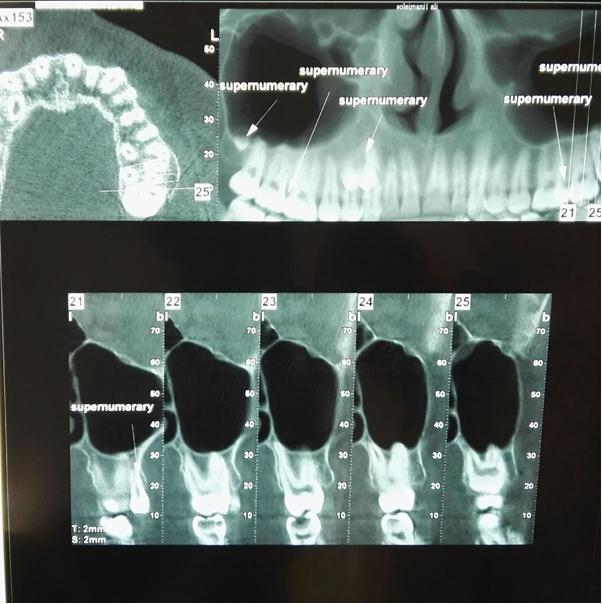
Fig2. Axial, cropped reconstructed panoramic and cross sectional CBCT views of the maxilla
Full-Text: (971 Views)
Introduction
Supernumerary teeth could be defined as the teeth in excess of the normal dentition (1). Such an overplus can also be accompanied by a loss of other teeth. For instance, 32 permanent teeth may be present with five mandibular incisors and only three mandibular premolars. It can be single or multiple, unilateral or bilateral, morphologically malformed or normal in shape and size, and erupted or impacted (2-4). Cases that involving one or two supernumerary teeth most commonly involve the anterior region of upper jaw, and after that the lower jaw premolar area (5). While multiple supernumerary teeth are present (>5), the most common place that affected could be the region of bicuspid teeth (6). Single supernumeraries occur in 76 to 86 percent of cases. Double supernumeraries occur in 12 to 23 percent of cases, and multiple supernumeraries in less than one percent (7-9).
The incidence of supernumerary teeth, according to the literatures, varies between 1.6 and 3.1 percent (10-13). Though they could be found in either the deciduous or permanent dentition, Clayton found them to be twice as often in the permanent dentition (11). They could be seen anywhere, nonetheless, there is a predilection to occur in the anterior maxillary area. Luten found 97 percent of supernumeraries were located in the anterior area while just three percent in the premolar region(13), whereas, Bodin and Thomsson found 10.9 percent of supernumerary teeth representing premolars, and 6.2 percent of the total number of supernumeraries were molar teeth. The most frequent cases were those with single supernumerary even though bilateral cases were seen. There was a higher frequency for males than females of nearly 2:1 with a higher incidence in the upper jaw in comparison with the lower jaw mentioned at between 6:1 to 11/1(12-15).
There is a number of published report of cases about the occurrence of multiple supernumeraries in the bicuspid teeth area but this anomaly is somewhat rare (16, 17).
The etiology of the supernumerary teeth still remains open to question. Phylogenetic process of atavism (evolutionary throwback) (18), dichotomy theory (splitting of the tooth bud) (19), hereditary and a combination of environmental and genetic factors (20) are among the probable theories that have been pronounced to explain the etiology of supernumerary teeth. The localized and independent hyperactivity of dental lamina could be the most accepted etiology for the supernumeraries' development (19). However, the presence of supernumeraries usually is a part of syndrome and developmental disorders such as Cleft palate and lip, Gardner's syndrome, Ehlers-Danlos syndrome, Cleidocranial dysostosis, Tricho-Rhino-Phalangeal syndrome, Ellis-Van Creveld syndrome, and Incontinentia Pigmenti. It has been reported that the prevalence of non-syndromic multiple supernumeraries is less than one percent (2, 21).
Mainly, supernumeraries could be categorized as either supplemental or rudimentary. Morphologically, supplemental teeth are similar to a normal tooth, but rudimentary teeth are small, conical, or tuberculate (22). In most cases, supernumerary premolars tend to be supplemental (23).
The purpose of this paper is to share radiological documents and assessments of a rare case of a large number of non-syndromic supernumerary teeth.
Case report
A 19-year-old Iranian male presented for an initial dental examination which involved taking panoramic radiograph. The patient had no complaint of pain, no sign of infection and was in good general health, with no other alterations. The patient has the history of bilateral ulnar polydactyly that was removed operatively at his early childhood. This bilateral ulnar polydactyly was not associated with syndactyly and polydactyly of the feet. On intraoral examination there were no abnormalities in the shape or size of the teeth or the relationship between the patient’s dental and chronological age. And also, there was no any other specific oral finding and relevant familial history of dental abnormalities. On clinical examination no craniofacial and skeletal anomaly related to supernumeraries (e.g. craniosynostosis, absence of clavicles, hypertelorism, ear deformity, etc.) was detected. The panoramic radiograph showed the presence of ten supernumerary teeth in all four quadrants (Fig. 1). On clinical examination it was found that all the permanent teeth including the third molars had erupted and the tooth number 36 had been extracted. CBCT (cone beam computed tomography) of the mandible and maxilla was taken to confirm the location of the supernumerary teeth and impact of these teeth on the adjacent teeth (Fig. 2, 3).
Supernumerary teeth could be defined as the teeth in excess of the normal dentition (1). Such an overplus can also be accompanied by a loss of other teeth. For instance, 32 permanent teeth may be present with five mandibular incisors and only three mandibular premolars. It can be single or multiple, unilateral or bilateral, morphologically malformed or normal in shape and size, and erupted or impacted (2-4). Cases that involving one or two supernumerary teeth most commonly involve the anterior region of upper jaw, and after that the lower jaw premolar area (5). While multiple supernumerary teeth are present (>5), the most common place that affected could be the region of bicuspid teeth (6). Single supernumeraries occur in 76 to 86 percent of cases. Double supernumeraries occur in 12 to 23 percent of cases, and multiple supernumeraries in less than one percent (7-9).
The incidence of supernumerary teeth, according to the literatures, varies between 1.6 and 3.1 percent (10-13). Though they could be found in either the deciduous or permanent dentition, Clayton found them to be twice as often in the permanent dentition (11). They could be seen anywhere, nonetheless, there is a predilection to occur in the anterior maxillary area. Luten found 97 percent of supernumeraries were located in the anterior area while just three percent in the premolar region(13), whereas, Bodin and Thomsson found 10.9 percent of supernumerary teeth representing premolars, and 6.2 percent of the total number of supernumeraries were molar teeth. The most frequent cases were those with single supernumerary even though bilateral cases were seen. There was a higher frequency for males than females of nearly 2:1 with a higher incidence in the upper jaw in comparison with the lower jaw mentioned at between 6:1 to 11/1(12-15).
There is a number of published report of cases about the occurrence of multiple supernumeraries in the bicuspid teeth area but this anomaly is somewhat rare (16, 17).
The etiology of the supernumerary teeth still remains open to question. Phylogenetic process of atavism (evolutionary throwback) (18), dichotomy theory (splitting of the tooth bud) (19), hereditary and a combination of environmental and genetic factors (20) are among the probable theories that have been pronounced to explain the etiology of supernumerary teeth. The localized and independent hyperactivity of dental lamina could be the most accepted etiology for the supernumeraries' development (19). However, the presence of supernumeraries usually is a part of syndrome and developmental disorders such as Cleft palate and lip, Gardner's syndrome, Ehlers-Danlos syndrome, Cleidocranial dysostosis, Tricho-Rhino-Phalangeal syndrome, Ellis-Van Creveld syndrome, and Incontinentia Pigmenti. It has been reported that the prevalence of non-syndromic multiple supernumeraries is less than one percent (2, 21).
Mainly, supernumeraries could be categorized as either supplemental or rudimentary. Morphologically, supplemental teeth are similar to a normal tooth, but rudimentary teeth are small, conical, or tuberculate (22). In most cases, supernumerary premolars tend to be supplemental (23).
The purpose of this paper is to share radiological documents and assessments of a rare case of a large number of non-syndromic supernumerary teeth.
Case report
A 19-year-old Iranian male presented for an initial dental examination which involved taking panoramic radiograph. The patient had no complaint of pain, no sign of infection and was in good general health, with no other alterations. The patient has the history of bilateral ulnar polydactyly that was removed operatively at his early childhood. This bilateral ulnar polydactyly was not associated with syndactyly and polydactyly of the feet. On intraoral examination there were no abnormalities in the shape or size of the teeth or the relationship between the patient’s dental and chronological age. And also, there was no any other specific oral finding and relevant familial history of dental abnormalities. On clinical examination no craniofacial and skeletal anomaly related to supernumeraries (e.g. craniosynostosis, absence of clavicles, hypertelorism, ear deformity, etc.) was detected. The panoramic radiograph showed the presence of ten supernumerary teeth in all four quadrants (Fig. 1). On clinical examination it was found that all the permanent teeth including the third molars had erupted and the tooth number 36 had been extracted. CBCT (cone beam computed tomography) of the mandible and maxilla was taken to confirm the location of the supernumerary teeth and impact of these teeth on the adjacent teeth (Fig. 2, 3).
Fig1. The panoramic radiograph showed the presence of ten supernumerary teeth in all four quadrants
Fig2. Axial, cropped reconstructed panoramic and cross sectional CBCT views of the maxilla
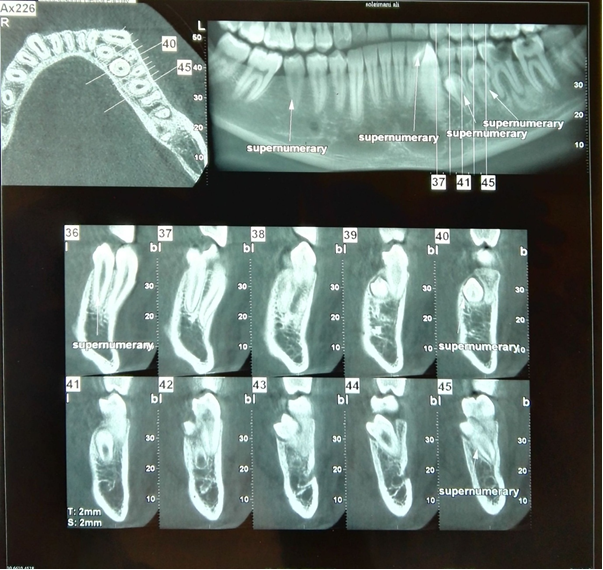
Fig3. Axial, cropped reconstructed panoramic and cross sectional CBCT views of the mandible
The first quadrant showed the presence of three supernumerary teeth. One of them was a distomolar (fourth molar), exhibiting a microdent tooth without complete root formation which lied in the right maxillary tuberosity at the apical region of the 18. A supernumerary premolar had buccally erupted between the 16 and 17. This tooth was normal in size and morphology as a premolar. Another supernumerary premolar was also found palatally to and at about the middle premolar as well. It seems that this supernumerary tooth had resorbed the palatal root of the 14. The gingiva around these teeth appeared healthy, with periodontal probing depths of 2 mm and no bleeding. There were also two supernumerary molars in second quadrant at the level of apical third of the roots of the 28. Both of these exhibit microdontia without complete root formation. These two supernumerary teeth seem to have close proximity with each other. One erupted supernumerary tooth was found in the second quadrant, buccal to and between the 26 and 27. These teeth had fully formed crown and root with normal morphology and size of a premolar. In the left mandibular premolar region there were three supernumerary teeth, all with fully formed crowns and roots. Two of these were unerupted and similar to normal premolars in size and morphology. One of them was between 35 and 36 lingually that resorbed lingual region of the root of 35 and mesial root of 36 at the middle third of it. The other was between 34 and 35 lingually and resorbed lingual part of the 34 and 35 in their root region too. Another erupted supernumerary tooth which found between 33 and 34 buccally exhibited the normal morphology and size as a canine. One supernumerary tooth was found in the right mandibular quadrant in the premolar region between 45 and 46. This erupted tooth had fully formed crown and root, and resembled the size and morphology of a normal premolar as well.
Discussion
The etiology of supernumerary teeth remains unclear, but several theories have been offered for it. The localized and independent hyperactivity of the dental lamina is the most accepted cause for the development of supernumerary teeth (2-24). Multiple supernumerary teeth without any syndromic association are very rare (6). An unerupted supernumerary tooth may be found by chance during radiographic examination, with no effect on adjacent teeth (2). If teeth are not causing any complications and are not likely to interfere with orthodontic tooth movement they could be radiographically observed every year. The patient needs to be informed about likely incoming problems and complications, such as migration and cystic change with damage to adjacent roots. It is reasonable to extract supernumeraries, if the patient does not accept such risks and problems. If supernumeraries are associated with the roots of permanent teeth, it may be logical to await full root development before removing the supernumerary teeth to decrease the chances of root damage (25).
The case that described here shows a sample of some features for cases with supernumeraries. It is indispensable to list and identify the teeth present clinically and radiographically before any diagnosis and treatment planning.
Supernumeraries usually are removed surgically, because of retention of permanent teeth in that area. A conservative approach is considered while the supernumeraries do not make change in the position, eruption, and integrity of the permanent dentition (26). Therefore, each case should be examined individually concerning retention of permanent teeth, tendency for cyst formation and malocclusion. The most common complications associated with the supernumeraries in the bicuspid teeth area are damage to neighboring teeth (13%t) and cyst formation (9%) (27). Some studies reported displacement, rotation, ectopic eruption, and malocclusion in their cases (28). But in our case, occlusion was normal and no discrepancies observed.
Conclusion
In cases with multiple impacted teeth or severe overlapping of impacted teeth, determining the relationships of teeth and the surrounding structures in 3D space is very difficult (29). Close observation with regular radiographic controls is recommended. CBCT is the best diagnostic imaging method currently available; it provides better resolution for hard tissues and also correctly localizes the retained teeth and determines their relationship with adjacent tissues.
Acknowledgements
Our special thanks go to members of the department of oral and maxillofacial radiology, faculty of dentistry, Ahvaz Jundishapur University of Medical Sciences.
Declarations
Ethics approvals and consent to participate: This manuscript has been approved by the research ethics committee of Ahvaz Jundishapour University of Medical Sciences. The code of Ethics is IR.AJUMS.REC.1399.395
The first quadrant showed the presence of three supernumerary teeth. One of them was a distomolar (fourth molar), exhibiting a microdent tooth without complete root formation which lied in the right maxillary tuberosity at the apical region of the 18. A supernumerary premolar had buccally erupted between the 16 and 17. This tooth was normal in size and morphology as a premolar. Another supernumerary premolar was also found palatally to and at about the middle premolar as well. It seems that this supernumerary tooth had resorbed the palatal root of the 14. The gingiva around these teeth appeared healthy, with periodontal probing depths of 2 mm and no bleeding. There were also two supernumerary molars in second quadrant at the level of apical third of the roots of the 28. Both of these exhibit microdontia without complete root formation. These two supernumerary teeth seem to have close proximity with each other. One erupted supernumerary tooth was found in the second quadrant, buccal to and between the 26 and 27. These teeth had fully formed crown and root with normal morphology and size of a premolar. In the left mandibular premolar region there were three supernumerary teeth, all with fully formed crowns and roots. Two of these were unerupted and similar to normal premolars in size and morphology. One of them was between 35 and 36 lingually that resorbed lingual region of the root of 35 and mesial root of 36 at the middle third of it. The other was between 34 and 35 lingually and resorbed lingual part of the 34 and 35 in their root region too. Another erupted supernumerary tooth which found between 33 and 34 buccally exhibited the normal morphology and size as a canine. One supernumerary tooth was found in the right mandibular quadrant in the premolar region between 45 and 46. This erupted tooth had fully formed crown and root, and resembled the size and morphology of a normal premolar as well.
Discussion
The etiology of supernumerary teeth remains unclear, but several theories have been offered for it. The localized and independent hyperactivity of the dental lamina is the most accepted cause for the development of supernumerary teeth (2-24). Multiple supernumerary teeth without any syndromic association are very rare (6). An unerupted supernumerary tooth may be found by chance during radiographic examination, with no effect on adjacent teeth (2). If teeth are not causing any complications and are not likely to interfere with orthodontic tooth movement they could be radiographically observed every year. The patient needs to be informed about likely incoming problems and complications, such as migration and cystic change with damage to adjacent roots. It is reasonable to extract supernumeraries, if the patient does not accept such risks and problems. If supernumeraries are associated with the roots of permanent teeth, it may be logical to await full root development before removing the supernumerary teeth to decrease the chances of root damage (25).
The case that described here shows a sample of some features for cases with supernumeraries. It is indispensable to list and identify the teeth present clinically and radiographically before any diagnosis and treatment planning.
Supernumeraries usually are removed surgically, because of retention of permanent teeth in that area. A conservative approach is considered while the supernumeraries do not make change in the position, eruption, and integrity of the permanent dentition (26). Therefore, each case should be examined individually concerning retention of permanent teeth, tendency for cyst formation and malocclusion. The most common complications associated with the supernumeraries in the bicuspid teeth area are damage to neighboring teeth (13%t) and cyst formation (9%) (27). Some studies reported displacement, rotation, ectopic eruption, and malocclusion in their cases (28). But in our case, occlusion was normal and no discrepancies observed.
Conclusion
In cases with multiple impacted teeth or severe overlapping of impacted teeth, determining the relationships of teeth and the surrounding structures in 3D space is very difficult (29). Close observation with regular radiographic controls is recommended. CBCT is the best diagnostic imaging method currently available; it provides better resolution for hard tissues and also correctly localizes the retained teeth and determines their relationship with adjacent tissues.
Acknowledgements
Our special thanks go to members of the department of oral and maxillofacial radiology, faculty of dentistry, Ahvaz Jundishapur University of Medical Sciences.
Declarations
Ethics approvals and consent to participate: This manuscript has been approved by the research ethics committee of Ahvaz Jundishapour University of Medical Sciences. The code of Ethics is IR.AJUMS.REC.1399.395
|
Type of Article: Case Report |
Subject:
General medicine
Received: 2020/02/25 | Accepted: 2020/05/1 | Published: 2020/06/18
Received: 2020/02/25 | Accepted: 2020/05/1 | Published: 2020/06/18
References
1. Schulze C. Developmental abnormalities of the teeth and jaws. In: Gorlin RJ, Goldman HM, eds. Thoma's oral pathology. St Louis: CV Mosby, 1970:112-22 [view at publisher] [Google Scholar]
2. Rajab LD, Hamdan MA. Supernumerary teeth: Review of the literature and a survey of 152 cases. Int J Paediatr Dent. 2002;12:244-54. [view at publisher] [DOI] [Google Scholar]
3. Gibson N. A late developing mandibular premolar supernumerary tooth. Aust Dent J. 2001;46:51-2. [view at publisher] [DOI] [Google Scholar]
4. Umweni AA, Osunbor GE. Non-syndrome multiple supernumerary teeth in Nigerians. Odontostomatol Trop. 2002;25:43-8. [view at publisher] [Google Scholar]
5. Mitchell L. Supernumerary teeth. Dent Update 1989;16:65-9. [view at publisher] [Google Scholar]
6. Yusof WZ. Non-syndromal multiple supernumerary teeth: literature review. J Can Dent Assoc 1990;56:147-9. [view at publisher] [Google Scholar]
7. So LLY. Unusual supernumerary teeth. Angle Orthod 1990;60:289-92. [view at publisher] [Google Scholar]
8. Scheiner MA, Sampson WJ. Supernumerary teeth: A review of the literature and four case reports. Aust Dent J. 1997;42:160-5. [DOI] [Google Scholar]
9. Zhu JF, Marcushamer M, King LD, Henry JR. Supernumerary and congenitally absent teeth: A literature review. J Clin Pediatr Dent. 1996;20:87-95. [view at publisher] [Google Scholar]
10. Grahnen H, Lindahl B. Supernumerary teeth in the permanent dentition. Odontol Rev 1961;12:290-4. [view at publisher] [Google Scholar]
11. Clayton JM. Congenital dental anomalies occurring in 3,557 children. J Dent Child 1956;23:206-8. [view at publisher] [Google Scholar]
12. Bodin I, Julin P, Thomsson M. Hyperdontia: I. Frequency and distribution of supernumerary teeth among 21,609 patients. Dentomaxillofac Radiol 1978;7:15-7. [DOI] [Google Scholar]
13. Luten JR. The prevalence of supernumerary teeth in primary and mixed dentitions. J Dent Child 1967;34:346-53. [view at publisher] [Google Scholar]
14. Bodin I, Julin P, Thomsson M. Hyperdontia: II. Supernumerary molars. Dentomaxillofac Radiol 1978;7:83-6. [view at publisher] [DOI] [Google Scholar]
15. Schulze C. Incidence of supernumerary teeth. Dent Abstr 1961;6:237. [Google Scholar]
16. Oehlers FAC. A case of multiple supernumerary teeth. Br Dent J 1951;90:211-2. [Google Scholar]
17. Lin TY. Seven supernumerary premolars. Report of a case. Br Dent J 1967;123:437-8. [view at publisher] [Google Scholar]
18. Smith JD. Hyperdontia: Report of a case. J Am Dent Assoc. 1969;79:1191-2. [DOI] [Google Scholar]
19. Liu JF. Characteristics of premaxillary supernumerary teeth: A survey of 112 cases. ASDC J Dent Child.1995;62:262-5. [view at publisher] [Google Scholar]
20. Brook AH. A unifying etiological explanation for anomalies of human tooth number and size. Archs Oral Biol. 1984;29:373-8. [view at publisher] [DOI] [Google Scholar]
21. Thumati P, David CM, Tiwari R. Non-syndromic multiple supernumerary teeth: A case report and review of literature. IJSS Case Reports & Reviews 2014;1(5):1-5. [Google Scholar]
22. Sykaras SN. Mesiodens in primary and permanent dentitions. Oral Surg. 1975;39:870-4. [DOI] [Google Scholar]
23. Hopcraft M. Multiple supernumerary teeth. Case report. Australian Dental Journal 1998;43:(1):17-19 [view at publisher] [DOI] [Google Scholar]
24. Solares, R, MI Romero. Supernumerary premolars: a literature review. Pediatr Dent 2004; 26:450-8. [view at publisher] [Google Scholar]
25. Ashish S. Diagnosis and management of supernumerary teeth. Dent Update 2008; 35: 510-520. [view at publisher] [DOI] [Google Scholar]
26. Koch a, Schwartz o, klausen b. indicators for surgical removal of supernumerary teeth in the premaxilla. Int j oral maxillofac surg 1986;15:273-81. [view at publisher] [DOI] [Google Scholar]
27. Hegde SV, Munshi AK. Late development of supernumerary teeth in the premolar region: a case report. Quintessence Int. 1996; 27:479- 81. [view at publisher] [Google Scholar]
28. Mason C, Rule DC, Hopper C. Multiple supernumeraries: the importance of clinical and radiographic follow-up. Dentomaxillofac Radiol. 1996; 25:109-13. [DOI] [Google Scholar]
29. Raupp S, Kramer PF, De Oliveira HW. Application of computed tomography for supernumerary teeth location in pediatric dentistry. J Clin Pediatr Dent 2008; 32:273-6. [view at publisher] [DOI] [Google Scholar]
Send email to the article author
| Rights and permissions | |
 |
This work is licensed under a Creative Commons Attribution-NonCommercial 4.0 International License. |
